The Global Challenge of Heart Disease
Daniel J. Penny
Jonathan R. Carapetis
Peter J. Hotez
“An epidemic of heart disease and stroke may be inevitable for the developing world in lieu of early action and the only hope to blunt its impact is to understand its origins, predict its magnitude and organize preventive and case management resources prior to its establishment” (1).
Introduction
The past 50 years have witnessed dramatic changes in the global epidemiology of cardiovascular disease. In most developed countries, deaths related to ischemic cardiovascular disease have progressively declined; acute rheumatic fever (ARF) and in turn, rheumatic heart disease (RHD) is becoming almost of historic interest and for many forms of congenital heart disease (CHD) formerly considered to be uniformly fatal, long-term survival can be ensured. It has been long recognized that neglected tropical diseases (NTDs), for example, Chagas disease, are a significant source of cardiac morbidity and mortality, but these conditions have been restricted to localized regions in the developing world.
Nonetheless, this developed-world view of the trends in cardiovascular mortality is far from representative of the global condition. By contrast, it is predicted that globally, deaths related to cardiovascular disease will continue to increase into the future. Rheumatic heart disease remains endemic in much of the developing world and in indigenous populations of even the most developed countries, while more than 90% of the world’s children still have no access to even the most basic care for CHD. Furthermore, it is now appreciated that, because of migration and increased ease of travel, diseases such as Chagas disease are now emerging in regions, where formerly they did not exist.
The specialist in pediatric cardiovascular disease can play a central role in positively influencing global cardiovascular-related mortality. Some of these issues will be considered here.
Global Burden of Cardiovascular Disease
One of the most detailed assessments of the impact of cardiovascular disease on global health is being led by an initiative known as the Global Burden of Disease Study 2013, based at the Institute for Health Metrics and Evaluation of the University of Washington. A recent analysis comparing the deaths from cardiovascular disease between 1990 and 2013 shows approximately a 40% increase in the number of cardiovascular deaths over the last 23 years (2). A snapshot of 2013 indicated that 17.3 million died from cardiovascular disease in that year, led by over 8 million people with ischemic heart disease and 6.5 million people from cerebrovascular disease (Table 80.1) (2).
Today, ischemic heart disease is the single leading cause of death globally, while cerebrovascular disease ranks number 3 (2). One of the key reasons for the rise of cardiovascular disease deaths globally, has been the disproportionate increase in cardiovascular disease in developing countries, especially the large middle-income countries, including the BRICS (Brazil, Russia, India, China, and South Africa), as well as Indonesia, Pakistan, and Bangladesh. Among the key factors for this increase has been expanding use of tobacco products and dietary changes. Indeed the rise in cardiovascular disease in the world’s low- and middle-income countries, is part of a larger trend in increases in noncommunicable diseases, possibly with a commensurate decrease in communicable disease.
CHD also exerts a large death toll. Overall, an estimated 246,100 neonates died of congenital anomalies (2).
However, an alternative narrative attributes some of the rise of cardiovascular disease in developing countries to neglected causes (3), which include rheumatic heart disease, but also neglected parasitic and tropical diseases, including Chagas disease, human African trypanosomiasis, toxoplasmosis, endomyocardial fibrosis (which in some instances has been partly attributed to helminth infections), hookworm infection, syphilis, tuberculosis, and HIV/AIDS (Table 80.2). Overall, both NCDs and NTDs account for the huge burden of cardiovascular disease in the developing world.
The Concept of the Epidemiologic Transition
In understanding the changing trends in regional cardiovascular mortality, it is useful to consider the concept of the “epidemiologic transition,” first formulated by Omran in 1971 (4). The epidemiologic transition may be considered as an evolutionary process within a society, which begins as the basic needs for water, food, and
shelter begin to be met. Life expectancy increases and the pattern of disease distribution within the community changes. Typically, the burden of infectious and parasitic diseases begins to decline and life expectancy rises further. Once life expectancy exceeds around 50 to 55 years, the number of deaths from cardiovascular causes tends to exceed those from infectious and parasitic disease (1).
shelter begin to be met. Life expectancy increases and the pattern of disease distribution within the community changes. Typically, the burden of infectious and parasitic diseases begins to decline and life expectancy rises further. Once life expectancy exceeds around 50 to 55 years, the number of deaths from cardiovascular causes tends to exceed those from infectious and parasitic disease (1).
TABLE 80.1 Estimated Number of Deaths Related to Cardiovascular Disease Worldwide | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||
TABLE 80.2 Global Cardiovascular Implications of Neglected Tropical Diseases | ||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||
At least four phases of the epidemiologic transition have been described. As a society advances through each stage of the transition, the nature of cardiovascular disease changes, as does its contribution to overall mortality (Table 80.3). In societies without even the most basic public health measures in place—those in the first, the so-called “Age of Pestilence and Famine”—the dominant cardiovascular diseases are rheumatic, as well as infectious and nutritional conditions (e.g., Chagas disease and beri-beri). As the society develops basic public health systems and undergoes the transition into the “Age of Receding Pandemics,” hypertensive heart disease and stroke increase, as cardiovascular disease assumes a greater proportion of overall mortality. Further development heralds the “Age of Degenerative and Human-Made Disease.” Ischemic heart disease and stroke increase further, typically occurring in relative young people. During the final phase of the transition, “The Age of Delayed and Degenerative Disease” cardiovascular disease still accounts for up to half of all deaths, but at advanced ages (5).
This model has proven to provide a useful framework for the study of the evolving epidemiology of disease. Nonetheless, it is important to emphasize that different populations within a single country, usually defined by socio-economic status sometimes linked to ethnicity (e.g., indigenous people living in wealthy countries, who are on the whole poorer than their nonindigenous countrymen), can be in different phases of the transition and so, a “one-size fits all” model of public health may not always suit. Thus, while it is reported that 43% of children in India are moderately or severely underweight (6), 22% of girls in affluent schools in New Delhi are overweight and 6% obese (7). Second, the speed with which a society transitions between phases can vary widely, so that a country still recovering from the burden of severe infections (e.g., HIV) may have to face the next wave of cardiovascular disease before resources can be put in place. Potentially, there may be a further phase of the epidemiologic transition; there is a growing epidemic of obesity, diabetes, and hypertension, the decline in smoking rates appears to be leveling off in some countries and it appears that adverse trends in risk factors may be reversing the progress made in the last half of the 20th century (8) (see Table 80.3).
The Impending Global Epidemic of Ischemic Cardiovascular Disease
In 2000, the United Nations in collaboration with key partners developed the Millennium Development Project (9), which aimed to reverse the poverty, hunger, and disease affecting billions. While the project appears to have had a profound positive impact on global mortality in a number of respects, it did not adequately address the major problem of noncommunicable diseases, of which cardiovascular disease is one (10). Indeed it has been predicted (11) that globally, deaths related to cardiovascular disease will increase from 16.7 million in 2002 to 23.3 million, of which more than 80% will occur in low- and middle-income countries, by 2030. As a result,
deaths related to cardiovascular disease would exceed those related to all communicable diseases combined. An ambitious target to reduce premature deaths from noncommunicable diseases by 25% by 2025 was endorsed by the World Health Organization at its 65th World Assembly in early 2012 (12). This initiative was heralded as a “game changer” by the World Heart Federation (13).
deaths related to cardiovascular disease would exceed those related to all communicable diseases combined. An ambitious target to reduce premature deaths from noncommunicable diseases by 25% by 2025 was endorsed by the World Health Organization at its 65th World Assembly in early 2012 (12). This initiative was heralded as a “game changer” by the World Heart Federation (13).
TABLE 80.3 The Relationship Between the Epidemiologic Transition and Cardiovascular Disease | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
Ischemic Cardiovascular Disease, Not Just a Disease of the Affluent and the Elderly
A traditional assumption has been that chronic noncommunicable diseases are diseases of the affluent and the elderly. More recent data refute this assumption (1). Although a study of more than 100 countries did indeed demonstrate that risk factors for ischemic cardiovascular disease increase as national incomes increase from very low levels, the relationships flatten, however, and eventually decline with further increases in income. Thus Body Mass Index increases up to a national income of about I$12,500 (international dollars) per capita for women and I$17,000 for men and the inflection point of serum cholesterol is at approximately I$18,000 (Fig. 80.1) (14). These observations are consistent with studies demonstrating that in a cohort of subjects screened for cardiovascular risk factors at a mean age of 46 years in Soweto, South Africa, 78% of subjects had at least one major risk factor for cardiovascular disease, while 55% of women and 23% of men were obese (15). It also appears that within South Africa and other countries, as gross national income increases, there has been a progressive drift in risk factor prevalence
over time from those within the higher to those within the lower socioeconomic classes (16).
over time from those within the higher to those within the lower socioeconomic classes (16).
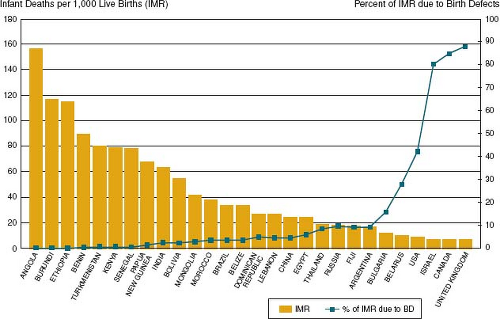 Figure 80.1 Relationship between infant mortality rate and percentage of infant deaths due to birth defects in the absence of known preventive services by country, 2004. (Data from personal communication, Bernadette Modell. Used with permission.) |
Accumulation of multiple risk factors within an individual also appears to be common in the developing world. For patients who attended a large cardiology unit in Soweto, 77% had more than 1 risk factor for ischemic cardiovascular disease. Of those with hypertension, for example, 38% also had hypercholesterolemia and 36% were smokers (17).
While currently ischemic cardiovascular disease in developed countries predominates in the elderly, it is projected that in South Africa for example, cardiovascular disease will impact four times more adults aged 35 to 64 than in the United States (see Fig. 80.1) (5). This will have a profound impact on the economy of developing countries (18). It has been estimated that in five countries surveyed (Brazil, India, China, South Africa, and Mexico), conservatively, cardiovascular disease will result in loss of at least 21 million years of future productive life annually (19).
Risk Factors for Cardiovascular Disease in Low- and Middle-Income Countries
Most of the current knowledge related to risk factors for ischemic cardiovascular disease is derived from populations of European origin. One important standardized case-control study examined risk factors for acute myocardial infarction in 52 countries representing every inhabited continent (the “Interheart” Study). It was observed that abnormal lipids, smoking, hypertension, diabetes, abdominal obesity, psychosocial factors, consumption of fruits, vegetable and alcohol, and lack of regular physical activity account for most of the risk of myocardial infarction worldwide, in both sexes and at all ages. It was therefore suggested that while priorities may differ between geographic regions because of variations in the prevalence of individual risk factors and economic circumstances, approaches to prevention can be based on similar principles worldwide (20).
The risk for ischemic cardiovascular disease may be modified in developing countries by a number of factors. The first is poverty and malnutrition. It is likely that maternal malnutrition may be of particular importance through its impact on the developing fetus, manifest through low birth weight. Globally, more than 20 million low–birth-weight infants are born annually. The incidence of low birth weight in developing countries is more than double (16.5%) that in the developed (7%), such that more than 95% of low–birth-weight infants are born in low- and middle-income countries (21). The impact of low birth weight on cardiovascular risk is likely to be profound and multifactorial. First, poverty and malnutrition during pregnancy may result in a low–birth-weight infant who is at risk of reduced physical and mental capacity, resulting in poverty in adulthood and the propagation of the vicious cycle of poverty (22). Second, the mismatch between fetal nutritional deprivation and later nutritional affluence may place individuals at particular risk for cardiovascular disease, via the so-called “fetal origins of disease” mechanism, as first expounded by Barker et al. (23). In a study, which examined the relationship between maternal energy consumption during pregnancy and potential cardiovascular risk in their offspring, carotid intima-media thickening (a surrogate marker of cardiovascular risk) was observed in obese 9-year olds, particularly those whose mothers had been in the lowest quartile of energy consumption during pregnancy (24). It thus appears that until nutritional affluence feeds through to improved maternal nutrition during pregnancy, at least one generation will be at particularly increased cardiovascular risk (25).
A second influence, which is likely to make an increasing contribution to cardiovascular risk in upcoming decades is HIV infection. Currently, it is estimated that there are more than 35 million people living with HIV (26). As access to highly-active retroviral therapies is increasing and HIV infection is becoming a more chronic illness, non-communicable diseases including cardiovascular disease are becoming an increasing source of morbidity (27,28). It has been estimated that HIV infection is associated with a 50% increase in the risk of an acute myocardial infarction beyond that explained by traditional risk factors (29). While as yet the pathogenic link between HIV and cardiovascular risk is unclear, it is likely to be a due to a combination of factors, including the effects of ongoing chronic inflammation, progressive immunologic dysfunction or possible the effects of the antiretroviral treatments themselves (30). It is likely that the impact will be most profound in middle- and low-income countries where more than 70% of HIV-positive patients live. It is also likely that children may be particularly susceptible because of potentially more years of life living with the condition and also possibly related to in utero exposure (31).
Managing the Impending Global Epidemic: A Focus on Children
The United States spends more than $45 billion on percutaneous coronary interventions (32) and $20 billion on lipid-lowering drugs (33) annually. It is not likely that the economies of the developing world will be able to support these expenses. Rather, if we are to optimally address the potential epidemic of ischemic cardiovascular disease in 2030, we will need to act now, focus on prevention, and address our attention to the youth (34,35).
The key principles and objectives for a global program to address the gaps in policy and research for noncommunicable diseases (including cardiovascular disease), were outlined by the World Health Organization (36) (Table 80.4). These overarching principles include the recognition that control strategies must be closely linked to the promotion and protection of human rights, that NCDs are a major challenge to social and economic development, that there needs to be equal access of opportunity to all members of the community and a strengthening of international cooperation, advocacy, and capacity. Of particular importance to the specialist in pediatric cardiovascular disease are the recommendations that health systems must be reoriented toward prevention rather than treatment, that exposure to modifiable risk factors including smoking needs to be reduced and that if these preventive strategies are to be successful, they need to be applied against the background of a “Life-Course Approach” (see Table 80.4).
As far back as 1961, Holman suggested that atherosclerosis is a pediatric problem (37). There is increasing evidence to justify the introduction of preventive strategies in childhood. Several studies clearly demonstrate that exposure to high levels of cardiovascular risk factors in childhood shows a significant relationship with later preclinical changes in early adulthood. (38). For example, risk factor burden at 9 years predicts increased carotid intima-media thickening in adulthood (39). In high-income countries, programs of dietary interventions have begun as early as infancy (40) and given that very few people initiate smoking or become habitual smokers after their teen years, a large number of community- and school-based programs to prevent smoking have focused on children in elementary and/or middle school. (41)
There is worrying evidence of significant accumulation of modifiable risk factors for cardiovascular disease in children in developing communities. In the “Wellbeing of Adolescents in Vulnerable Environments (WAVE) Study, 32.5% of adolescents were already currently using cigarettes, 30.8% of these were consuming more than 10 per day and the average age at which children smoked their first cigarette was 14 years (42). The prevalence of childhood overweight and obesity is increasing in developing countries, in tandem with the increases in the developed world. In a study of primary school females in Zululand 9% were overweight and 3.8% obese (43). A study of 15- to 24-year olds in South Africa demonstrated that 30% of females were overweight or obese and 46% were “physically
inactive” (44). While it appears that adolescent girls in South Africa are aware of the benefits of healthy eating, they experience limited access to healthy food (45). In a further study of rural South African children, only 26% met international health guidelines of 60 minutes per day of moderately vigorous physical activity, with low levels of activity being particularly evident on those of low socioeconomic status (46).
inactive” (44). While it appears that adolescent girls in South Africa are aware of the benefits of healthy eating, they experience limited access to healthy food (45). In a further study of rural South African children, only 26% met international health guidelines of 60 minutes per day of moderately vigorous physical activity, with low levels of activity being particularly evident on those of low socioeconomic status (46).
TABLE 80.4 Principles and Objectives Toward Reducing the Global Burden of Noncommunicable Diseases as Developed by the World Health Organization | ||||
|---|---|---|---|---|
|
If we are to prevent the global epidemic of acquired cardiovascular disease there is an urgent need to develop preventive programs in low- and middle-income countries. They need to be based on a life-stages approach and begin in childhood. They will need to be tailored to individual populations, so that they are evidence-based and empower local communities. The specialist in pediatric cardiovascular disease can make an important contribution to these programs.
Rheumatic Heart Disease
A comprehensive review of the clinical aspects of RHD is included elsewhere in this text. This section will consider some of its global implications.
Globally, interest in RHD has waxed and waned over the past 70 years since T. Duckett Jones’ pivotal paper outlining the diagnostic criteria for ARF in 1944 (47). The mid-20th century witnessed a surge of interest, particularly in the United States, during which we learned most of what we now know about primary and secondary prevention. Interest in RHD appeared to wane in the wealthy countries in the 1970s and 1980s, in parallel with reducing rates of disease. It was during this era that the problem of RHD in developing countries became increasingly recognized and, led by the World Health Organization, a global program of control was established in 22 countries in the 1980s. This program was abandoned by the turn of the millennium. Since then a new and exciting era has begun with emergence of influence from regions where RHD remains a major problem. Research, advocacy and policy are now dominated by individuals working in low- and middle-income countries (and some high-income countries where RHD remains hyper-endemic), with some coordination and leadership being provided by the World Heart Federation.
Epidemiology of Rheumatic Heart Disease
The 20th century witnessed a dramatic reduction in the occurrence of ARF and RHD in the high-income regions of North America and Europe. As a result, apart from a number of rare, local epidemics, ARF and RHD are virtually eliminated in these regions. Although clearly, the introduction of penicillins has contributed to these reductions, it is likely that an even greater contribution was made by economic and socio-political changes in these countries. Thus, for example, it was noted that dramatic reductions in the incidence of ARF in Denmark preceded the introduction of penicillin (48).
Nonetheless ARF and RHD continue to be endemic in many middle- and low-income countries and within certain indigenous populations of higher-income countries, for example, the Aboriginal populations of Australia and the Maori population of New Zealand.
The true size of the problem of ARF and RHD remains difficult to estimate. In 2005 a report on the global burden of group A streptococcal disease, commissioned by the World Health Organization, calculated the prevalence of RHD, incidence of ARF and incidence of new cases of RHD, based on population data published between 1985 and 2005 across multiple regions. The study found an overall global burden of 471,000 annual cases of ARF, with the incidence in children aged 5 to 15 years ranging from 10 cases per 100,000 in industrialized countries to 374 cases per 100,000 in the Pacific region. There were estimated to be at least 15.6 million prevalent cases of RHD worldwide with 282,000 new cases and over 233,000 deaths per year (49). As a result, it was estimated that in the late 1990s RHD was the most common cardiovascular disease in those aged less than 25 years worldwide. A subsequent systematic review, which added more studies highlighted the wide global variation in the incidence and prevalence of ARF and RHD and suggested that the greatest burden of disease was in sub-Saharan Africa (50). The highest mortality rates from the two diseases were in the indigenous populations of Australia (23.8 per 100,000). The Global Burden of Disease Study estimated that, in 2010, there were more than 34 million people with RHD, resulting in more than 10 million disability-adjusted life years lost and 345,000 deaths (51).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


