(1)
Department of General surgery, Fuwai Hospital, Beijing, China
5.1 Coronary Artery Anatomy
The coronary artery anatomy includes: (1) the left main coronary artery (LMCA), also known as the left coronary artery (LCA); (2) the left anterior descending artery (LAD) and its main branches; (3) the left circumflex artery (LCx) and its main branches; (4) the right coronary artery (RCA); and (5) the posterior descending artery (PDA) (Figs. 5.1a, b). The coronary vein is parallel to the artery (Figs. 5.2a–c). It merges into the coronary sinus, and all drain into the RA. The LCA originates from the left aortic sinus, whereas the RCA originates from the right aortic sinus above the AV (Figs. 5.3 and 5.4).
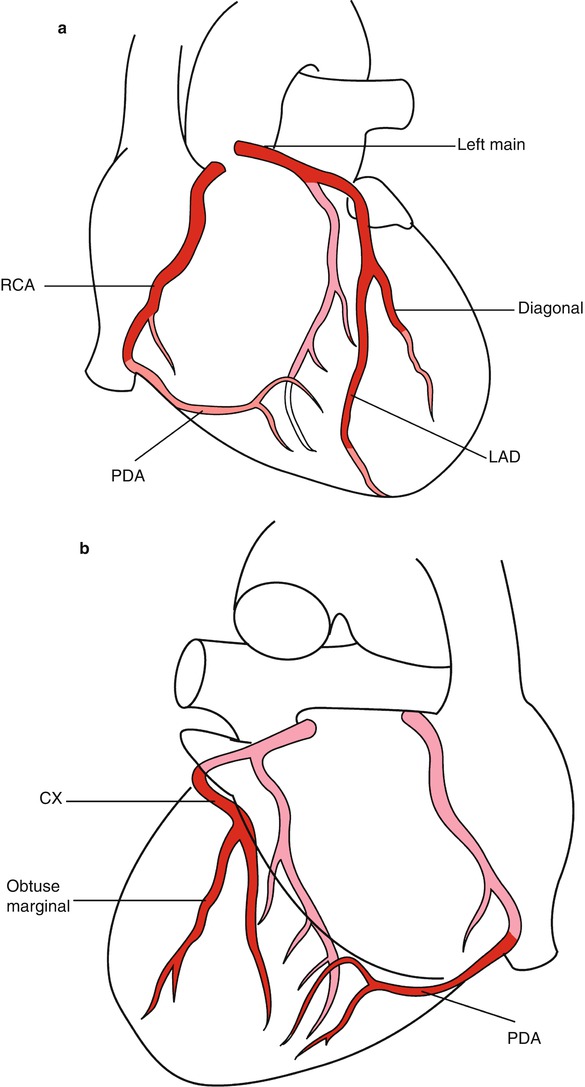
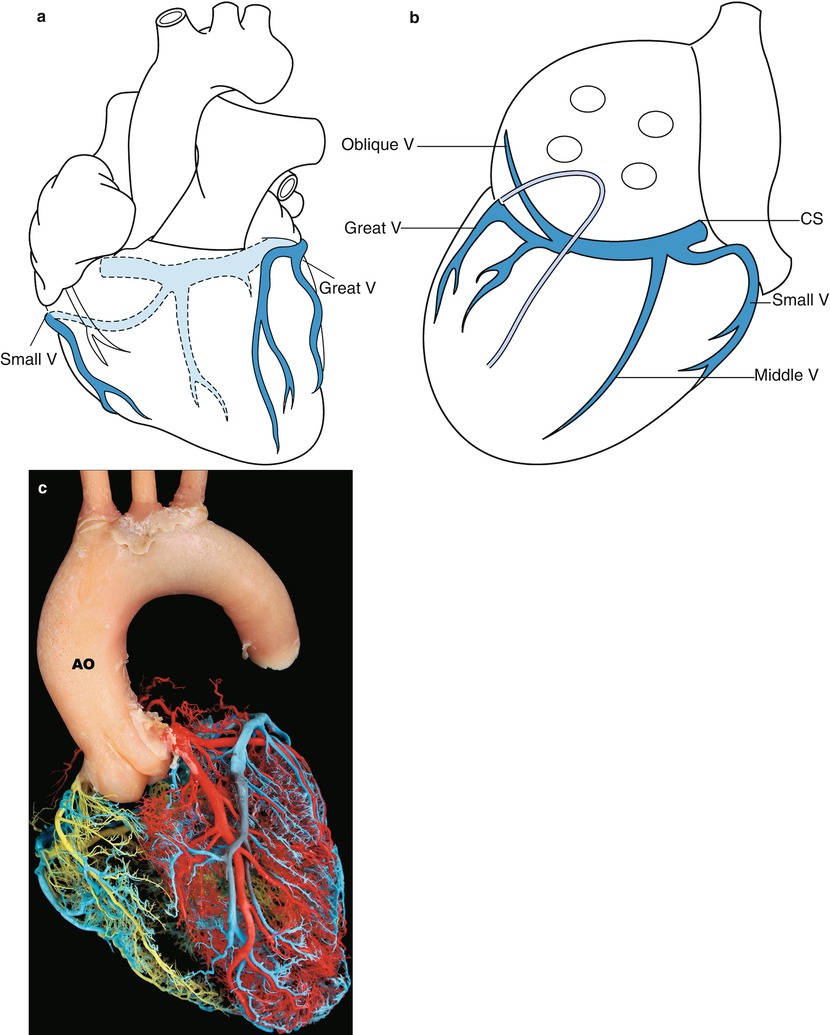
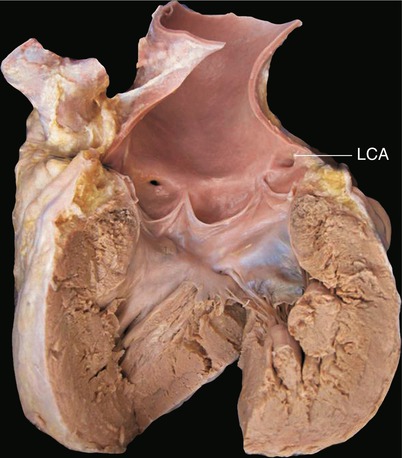
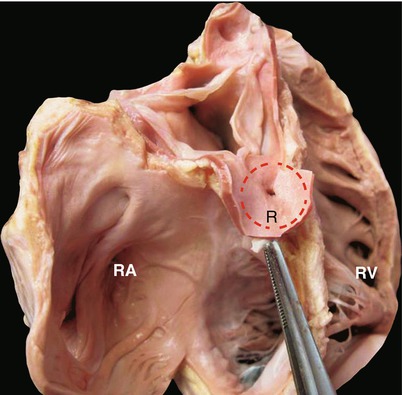
Fig. 5.1
(a) Coronary artery anatomy position, projecting from the front view. Deep red shade shows the anterior of the heart; light shade shows area behind the heart. The LAD is located in the left front portion. The heart is easily exposed by either a median sternotomy or a small incision on the left side of the chest. Minimally invasive techniques are used commonly for coronary artery bypass at this branch. Because it contains no giant branch of the LAD, the LV provides an ideal site for making a left ventricular incision. (b) Back projection of the coronary artery. Deep red shade indicates the LCx. The obtuse marginal branch (OM), the posterior descending branch, runs from the back of the heart. Exposing the branches at the back of the heart is more difficult in bypass surgery. LCx bypass is covered by the left atrial appendage. Caution must be exercised to avoid tearing the LAA, which may damage the LCx and cause fatal hemorrhage during the operation
Fig. 5.2
(a) Front positive, coronary venous projection. The deep blue branches indicate the great cardiac vein. On the right is the small cardiac vein. The vessels colored in light blue are the cardiac dorsal heart vein and coronary sinus. (b) Back projection of the heart coronary vein. The middle vein (middle V), the oblique vein (oblique V) of Marshall on the atrial posterior wall, and the coronary sinus (CS) in the atrioventricular groove are seen entering together into the RA. The oblique vein without full degradation becomes the thick left SVC, which may influence the cardiac operation under direct vision. The coronary sinus is the site for retrograde perfusion and for insertion of the catheter for interventional treatment. (c) Coronary artery. AO ascending aorta (from Zhong Shizhen academician)
Fig. 5.3
Position of the coronary artery ostia. The LV and the aorta are opened, revealing two coronary artery openings. The LCA is opened slightly higher, at the junction of the upper edge of the sinuses. The RCA is opened in the aortic sinus. The ventricular septal section is between the LCA and the RCA, as shown. Hypertrophy of the LV can cause stenosis of the outflow tract. Dredging the septal outflow tract can injure the coronary artery opening
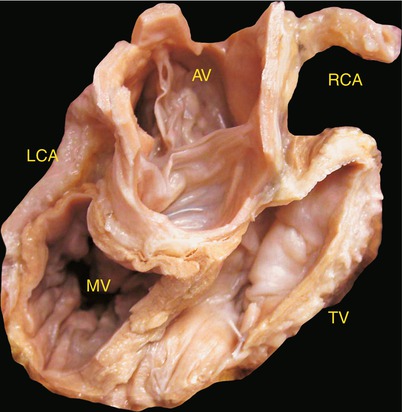
Fig. 5.4
Coronary artery ostia and aortic valve leaflets. The RA, the right ventricular anterior wall, and the aortic wall have been removed. The three aortic valve leaflets are fully deployed. The opening of the coronary artery is in the sinus pipe junction and near the valve junction. In an aortic root replacement operation, the coronary artery often needs to be reimplanted in an artificial vascular graft. A coronary artery opening together with the surrounding of the aortic wall is often dissociated with a button-type cutting. If the AV is to be preserved, care must be taken to avoid damaging the valve leaflet when freeing the coronary artery ostium. The dotted line represents the button tangent. L left coronary ostium, R right coronary artery ostium, RA right atrium, RV right ventricle
5.1.1 The Left Main Coronary Artery
The LMCA originates from the left coronary sinus in the ascending aorta (Fig. 5.5). The LMCA is short, running along the main pulmonary artery after the LAA and extending under the left atrioventricular groove (Figs. 5.6 and 5.7). The LMCA is embedded in fat and is covered by the LAA (Figs. 5.6 and 5.7). The LMCA bifurcates into two or three branches: the LAD, which runs along the anterior interventricular sulcus; the LCx, which runs along the left atrioventricular groove; and a branch between these two branches that becomes the intermediate branch (Fig. 5.8). The LAD, which is adjacent to the pulmonary artery (Figs. 5.6 and 5.9), crosses the apex and meets with the posterior interventricular groove, also called the PDA, in the posterior interventricular groove. The anterior main descending artery enters the apex as a single vessel and later grows into a diagonal branch with numerous septal branches (Fig. 5.10). The proximal LAD is covered by fat tissue on the heart’s surface. In most people, the proximal LAD is located in the inner layer of the pericardium. In a minority of patients with the anterior descending branch running within the myocardium, the ventricular contraction may compress the anterior descending artery and block the blood flow. The LCx runs along the left atrioventricular groove and has numerous left ventricular branches that bifurcate from it before it arrives at the apex (Fig. 5.11a, b). The ventricular branches supply the blood of the posterior wall of the LV (Fig. 5.12a).
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
