Teratoma
Presentation
A 32-year-old woman is referred to you by her primary care physician with complaints of chest discomfort for the past 2 weeks. She is otherwise a healthy, nonsmoking woman with no significant past medical history. Physical examination is unremarkable. The patient presents to your office with the following chest x-rays.
▪ Chest X-rays
 Figure 57-1 |
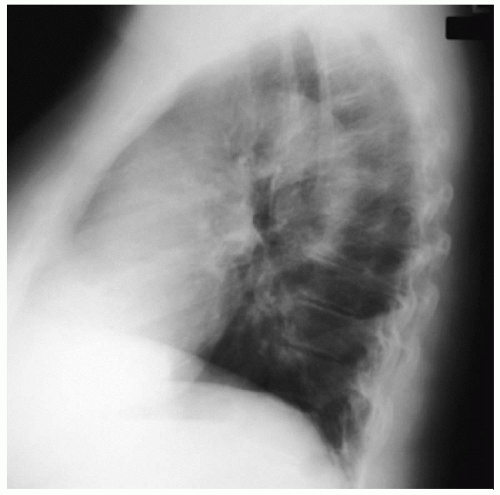 Figure 57-2 |
Chest X-ray Report
The chest x-rays demonstrate a large mass in the left chest. The left heart border is obscured by the mass. On the lateral x-ray, the mass is anterior to the heart. There are no lesions in the lung fields, and there is no evidence of pleural effusion.
Recommendation
The computed tomography (CT) scan is an accurate and reliable method to evaluate the mediastinum and lungs. A standard protocol for CT scanning of the chest includes contiguous images from the lung apices to the adrenal glands with inclusion of the liver. Intravenous contrast is recommended to define vascular structures in the chest and their relationship to any detected abnormalities.
▪ CT Scan
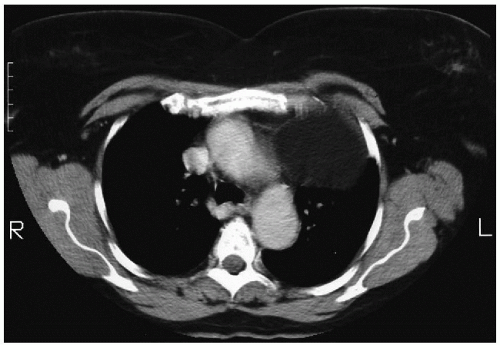 Figure 57-3 |
CT Scan Report
The CT scan demonstrates a left-sided anterior mediastinal mass in proximity to the arch of the aorta. The mass appears to be well circumscribed with a cystic component. There is no obvious invasion of mediastinal structures or of the adjacent lung parenchyma. The lung fields are free of abnormalities, and there is no pleural effusion. The liver and adrenals are normal. Calcification is noted in the mass.
Recommendation
Magnetic resonance imaging (MRI) can further delineate the relationship of the mass to adjacent vascular structures. MRI of the chest is not particularly beneficial for evaluating the lung parenchyma but does provide excellent soft tissue characterization along with vascular enhancement.



