The aortorenal anastomoses should usually be performed using interrupted monofilament sutures. However, a continuous suture may be used in older adolescents with large renal arteries. Most implantations of the renal artery will be into a normal infrarenal segment of the aorta (Figure 1). Medial mobilization of the kidney may be necessary to ensure that there is no tension on the implanted renal artery. A renal artery branch or accessory renal artery beyond its stenotic segment may also be implanted into a nondiseased adjacent main or segmental renal artery. This also involves spatulation of the segmental vessel and completion of the anastomosis using monofilament sutures (Figure 2). A renal artery may be implanted into the superior mesenteric artery when implantation elsewhere is deemed hazardous. The internal iliac artery is favored as a conduit when a pediatric renal bypass is undertaken (Figure 3). The excised internal iliac artery usually includes its distal branches, which are incised to create a large common orifice for the aortic anastomosis. The distal renal artery–to–iliac artery graft anastomoses should be completed following spatulation of both the iliac artery and renal artery to increase the anastomotic circumference. Such an ovoid anastomosis is less likely to develop a late stricture. In very young children with small arteries, the anastomoses should be completed with interrupted sutures, although a continuous suture may be used in reconstructing larger renal arteries. Stenoses of multiple small renal arteries can require approximation of these vessels to each other to form a larger common orifice to which an aortorenal graft can be anastomosed.
Surgical Treatment of Renovascular Hypertension in Children
Operative Therapy
Types of Surgery
Renal Artery Implantation
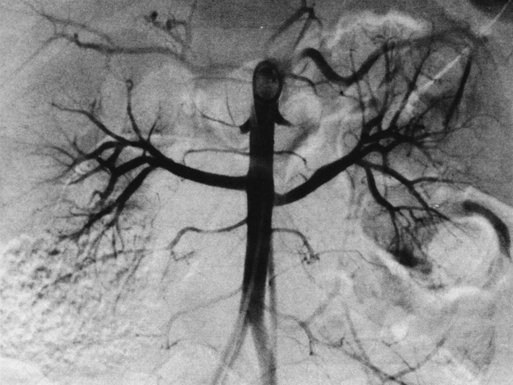
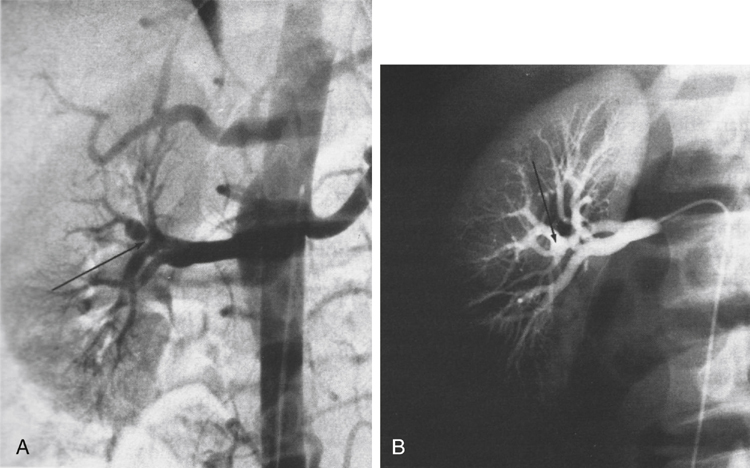
Aortorenal Bypass

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Surgical Treatment of Renovascular Hypertension in Children
