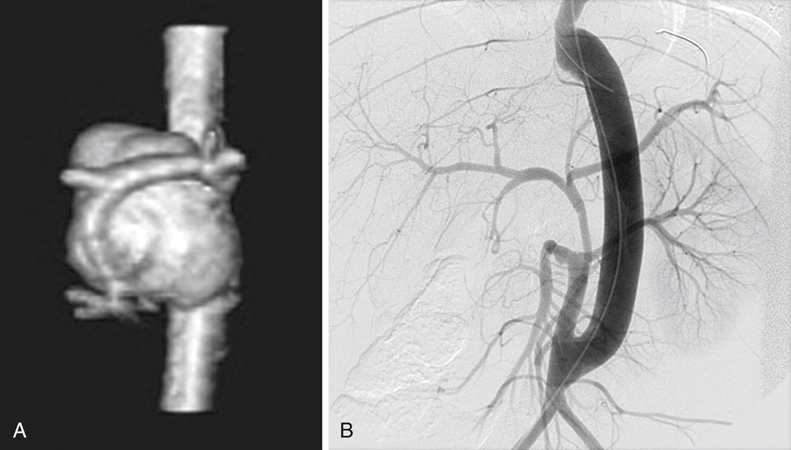
Jonathan L. Eliason, Enrique Criado, Dawn M. Coleman and James C. Stanley Infectious AAAs account for a third of aortic aneurysms reported in children. Such aneurysms are most commonly associated with umbilical artery catheterizations (UACs), with the need for repeated insertion or prolonged use of UAC resulting in increased risk. These AAAs are typically saccular, and rupture is the most serious sequela. They typically manifest in the newborn period, and more than 75% are associated with a Staphylococcus aureus or Staphylococcus albus infection, although polymicrobial infections are not rare. Their distribution is variable. More than half of these aneurysms affect the abdominal aorta, but the thoracic aorta and iliac vessels may also be involved (Figure 1). Tuberous sclerosis is an autosomal dominant genetic disorder in which hamartomas in multiple organ systems are the dominant theme. Central nervous system involvement is common, and children often experience learning difficulties and seizure disorders. Renal, pulmonary, skin, or other organ systems may also be affected. Although uncommon, the association with aneurysms has been well described. The majority of aortic aneurysms are abdominal, and thoracic aortic involvement is less common (Figure 2). The age at AAA diagnosis is variable, but instances of rupture and death are known to have occurred in infancy and childhood.
Surgical Treatment of Pediatric Abdominal Aortic Aneurysms
Etiologies

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine
