Supraventricular Arrhythmias and Atrial Fibrillation
Edgar Argulian
Dan G. Halpern
Emad F. Aziz
Eyal Herzog
Most common supraventricular arrhythmias encountered in the cardiac care unit (CCU) are sinus tachycardia and atrial fibrillation. The current chapter focuses on the general approach to narrow QRS complex tachycardias followed by the description of common forms of supraventricular tachycardias (SVTs) with a special emphasis of atrial fibrillation. The algorithms described in the chapter apply to the most common clinical scenarios and do not intend to be all-inclusive or highly specific.
SVTs usually present with a narrow QRS complex (<120 milliseconds) on ECG because of the normal sequence of ventricular activation using the His-Purkinje system. Occasionally, SVTs present with a wide QRS complex (≥120 milliseconds) because of the following reasons: preexisting conduction abnormalities (e.g., bundle branch block), rate-related aberrant conduction, or conduction using an accessory pathway. In those cases, differentiation from ventricular tachycardia can be challenging, and it is discussed in details in Chapter 17.
GENERAL APPROACH TO NARROW QRS COMPLEX TACHYCARDIAS
HEMODYNAMIC IMPACT
Patients presenting with narrow QRS complex tachycardias should be assessed for symptoms potentially attributable to the arrhythmia. These include hypotension, poor peripheral perfusion, altered mental status, shortness of breath, and chest pain. Although commonly well tolerated by otherwise healthy individuals, SVTs can have a significant hemodynamic impact on patients with cardiac comorbidities such as coronary artery disease, valvular diseases, and congestive heart failure. Before attributing hemodynamic instability to the arrhythmia, the underlying precipitants should be thought. For example, sepsis or pulmonary embolism in a patient with atrial fibrillation can be the driver of the rapid ventricular response. If SVT is thought to be the cause of hemodynamic instability, immediate treatment such as electrical cardioversion is warranted. One should keep in mind that sinus tachycardia is almost always a compensatory response, and it should not be considered the cause of hemodynamic instability. The underlying cause of sinus tachycardia (such as myocardial ischemia, congestive heart failure, etc.) should be identified and addressed.
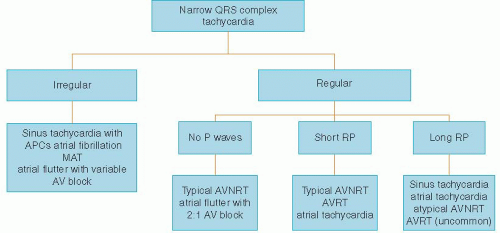 Figure 16.1. General approach to narrow QRS complex tachycardias. APC, atrial premature complex. |
REGULARITY OF THE RHYTHM
After determination of the hemodynamic impact of the arrhythmia, the 12-lead ECG should be inspected for regularity of QRS complexes (Figure 16.1). This allows rapid differentiation into two major categories: irregular rhythms and regular rhythms.1,2
Irregular rhythms should be further inspected for the presence and morphology of P waves. Atrial fibrillation is the most common irregular tachycardia, and it has no identifiable P waves. One must remember that atrial fibrillation with a very fast heart rate may appear regular, and careful inspection and
heart rate slowing maneuvers can help to disclose irregularity. Multifocal atrial tachycardia (MAT) has identifiable P waves indicative of atrial activity, but there is no single dominant focus (unlike sinus tachycardia with frequent atrial premature complexes). By definition, three different P-wave morphologies should be present on a single ECG with a heart rate exceeding 100 beats per minute (bpm) to diagnose MAT. Occasionally, atrial flutter presents as irregular tachycardia because of variable atrioventricular (AV) block.
heart rate slowing maneuvers can help to disclose irregularity. Multifocal atrial tachycardia (MAT) has identifiable P waves indicative of atrial activity, but there is no single dominant focus (unlike sinus tachycardia with frequent atrial premature complexes). By definition, three different P-wave morphologies should be present on a single ECG with a heart rate exceeding 100 beats per minute (bpm) to diagnose MAT. Occasionally, atrial flutter presents as irregular tachycardia because of variable atrioventricular (AV) block.
Regular rhythms should be further analyzed for the presence of P waves as outlined below. Paroxysmal SVTs are a group of arrhythmias in this category that are intermittent in nature and commonly start and terminate abruptly. These include AV node reentrant tachycardia (AVNRT), AV reentrant tachycardia (AVRT), and unifocal atrial tachycardia.
ABSENCE OF P WAVES IN LIMB LEADS
Identification of P waves is essential in further characterization of regular narrow QRS complex tachycardias. It requires familiarity and experience in ECG interpretation since P waves can be subtle and superimposed on other waves.1 Absence of identifiable P waves usually means that the atrial and ventricular activations are occurring almost simultaneously and P waves are completely buried within the QRS complex. The typical cause for such supraventricular arrhythmia is AVNRT with other causes (such as unifocal atrial tachycardia) being rare.
AVNRT develops in individuals with peculiar electrophysiologic (EP) properties of the AV node called dual AV node physiology. Within the AV node or in its proximity, there are two pathways having different conduction properties and refractoriness: fast pathway and slow pathway. As a result, an impulse can circulate between those pathways creating a regular arrhythmia at the rate of 130 to 250 bpm. Typically, the impulse travels down the slow pathway and up the fast pathway leading to simultaneous (no identifiable P waves) or almost simultaneous (P wave slightly after QRS complex) atrial and ventricular activation. Uncommonly, the impulse travels down the fast pathway and up the slow pathway (atypical AVNRT) leading to QRS complexes preceded by P waves.
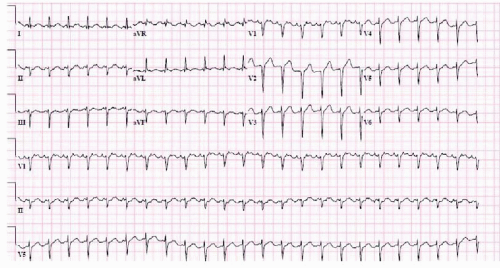 Figure 16.2. Atrial flutter with 2:1 AV block. Note F waves as undulations of the baseline in the inferior leads (II, III, avF) and small positive deflections in lead V1 (two per each QRS complex). The ventricular rate is regular at 142 bpm. |
Atrial flutter is an atrial macroreentrant rhythm, which is usually located in the right atrium with a counterclockwise circuit around the tricuspid valve (typical atrial flutter). The atrial rate is close to 300 bpm (240 to 340 bpm) typically conducting through the AV node with 2:1 block. Therefore, the ventricular rate is most commonly regular and close to 150 bpm. Any SVT with the ventricular rate close to 150 bpm should be specifically inspected for atrial flutter! On surface ECG, there are no P waves. Instead, “sawtooth” undulations of the baseline (F waves) are present in inferior leads (II, III, avF). In V1, small positive deflections are seen (two per each QRS complex). One should know that identification of F waves can be challenging because they are commonly obscured by other waves (Figure 16.2).
RP INTERVAL
If P waves are identified, the relationship between R wave and P wave should be determined. If the RP interval is less than one-half of the RR interval, the tachycardia is called a short RP tachycardia, otherwise it is a long RP tachycardia (Figure 16.1). Typical AVNRT is a common form of short RP tachycardia as described above. AVRT is another common form of short RP tachycardia.
AVRT develops in patients with an accessory pathway, an extranodal tissue that electrically connects the atrium with the ventricle bypassing the AV node. The pathway can manifest on baseline ECG as a Wolff-Parkinson-White (WPW) pattern if it conducts in both antegrade and retrograde directions. Some pathways conduct only retrograde (from the ventricle to the atrium). They are called concealed because they are not recognized on the baseline surface ECG. Typically, AVRT results from an impulse traveling down the AV node and up the accessory pathway (orthodromic AVRT). Therefore, orthodromic AVRT is a narrow QRS complex, short RP tachycardia resembling AVNRT. On average, the RP interval is slightly longer with AVRT compared with AVNRT (P wave is seen on top of ST segment as opposed to the end of QRS complex), but the difference is usually subtle. Uncommonly, AVRT results from an impulse traveling down the accessory pathway and up the AV node (antidromic AVRT). Antidromic AVRT is a wide complex, not a narrow complex tachycardia!
P-WAVE MORPHOLOGY
P-wave morphology assessment helps in further differential diagnosis of narrow QRS complex tachycardias. Sinus P waves are positive in lead II and negative in lead AVR. Retrograde P waves are always negative in inferior leads (II, III, avF) and commonly positive in V1. P waves originating from different foci in atria can have variable morphology including one closely mimicking sinus P waves (e.g., the rhythm originating from the crista terminalis). Therefore, comparison with the baseline ECG for P-wave morphology and documentation of the abrupt onset/termination is useful in differentiating long-RP tachycardias because of ectopic atrial activity from sinus tachycardia. AVNRT is always associated with retrograde P waves; any other morphology excludes AVNRT. AVRT can occasionally present with nonretrograde P-wave morphology depending on the location of the accessory pathway.
TRANSIENT SLOWING OF AV CONDUCTION
Transient slowing of AV conduction is essential in the differential diagnosis and acute treatment of SVTs.3 It is accomplished by bedside vagal maneuvers (such as Valsalva and carotid sinus massage) or if those are ineffective with medications (most commonly adenosine, sometimes β-blockers and calcium channel blockers). Before performing carotid sinus massage, check for contraindications such as history of cerebral vascular disease, recent myocardial infarction, or carotid bruits. Never perform bilateral carotid sinus massage. As adenosine has a very short half-life, it is given as a rapid intravenous push followed by saline infusion. The initial dose of adenosine is 6 mg (lower if using a central venous line), which can be followed by 12 mg if no response is seen. Adenosine can precipitate transient atrial fibrillation in up to 12% of patients that is potentially dangerous in patients with known WPW syndrome.4 Ventricular fibrillation and transient asystole in response to adenosine administration are rare. Patients should be warned that side effects (such as flushing, chest tightness, and shortness of breath) are very common but short lasting. Table 16.1 outlines the common responses to the transient slowing of AV conduction that help in differential diagnosis. Arrhythmias that use the AV node in the reentry circuit (such as AVNRT and AVRT) commonly terminate with the slowing of the AV nodal conduction. Other arrhythmias can slow down helping identification of the abnormal rhythm.
TABLE 16.1 Response of Narrow QRS Complex Tachycardias to the Transient Slowing of AV Nodal Conduction by Vagal Maneuvers or Mediations (e.g., Adenosine) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
LONG-TERM MANAGEMENT OF PAROXYSMAL SVTS
Patients with infrequent episodes of AVNRT that are well tolerated can be managed by AV node blocking medications (such as β-blockers or nondihydropyridine calcium channel blockers). In patients with frequent episodes of AVNRT or poorly tolerated episodes, catheter ablation is usually safe and effective. Catheter ablation should be strongly considered in patients with AVRT and WPW syndrome.
MAT is most commonly seen in the setting of advanced lung disease. It is also associated with some structural heart diseases and congestive heart failure. It requires rate control and management of the underlying condition. The former is commonly achieved by calcium channel blockers or β-blockers if there are no contraindications. Unifocal atrial tachycardias can be managed by rate control using AV node blocking medications. Occasionally, antiarrhythmic medications or catheter ablation is required.
ATRIAL FIBRILLATION
Atrial fibrillation is a common arrhythmia affecting 1% to 2% of general population. The prevalence increases dramatically with age affecting as many as 5% to 15% at the age of 80 years.5,6 Therefore, it is commonly encountered in hospitalized patients, especially in the CCU. Atrial fibrillation is strongly associated with both the risk and severity of stroke. It is also associated with higher all-cause mortality and rates of hospitalizations compared with normal sinus rhythm.
RECOGNITION
Atrial fibrillation is characterized by disorganized atrial activity exceeding 300 bpm. This results in the loss of effective atrial contraction and typically a rapid ventricular response. Atrial fibrillation is recognized on the surface ECG as an irregularly irregular rhythm with no distinct P waves (Figure 16.3). Sometimes signs of regular atrial activity are seen in lead V1. Ventricular rates during atrial fibrillation are usually in the range of 90 to 160 bpm. A slow ventricular rate without AV node blocking medications may indicate conduction system disease. Regular and slow ventricular response is seen in patients with atrial fibrillation who are in complete heart block. Very fast rates (>200 bpm) are also unusual because of concealed conduction in the AV node. They can be seen in the
states of significant catecholamine excess or in patients with an accessory pathway. One should recognize that atrial fibrillation is commonly an intermittent arrhythmia, at least early in the natural course of the disease. When clinically suspected, a long telemonitoring may be required for the correct diagnosis.
states of significant catecholamine excess or in patients with an accessory pathway. One should recognize that atrial fibrillation is commonly an intermittent arrhythmia, at least early in the natural course of the disease. When clinically suspected, a long telemonitoring may be required for the correct diagnosis.
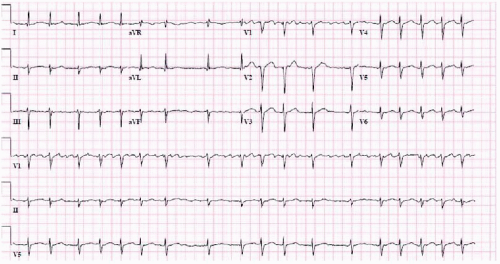 Figure 16.3. Atrial fibrillation. Note irregularly irregular and rapid ventricular response. Coarse fibrillatory waves can be best seen in lead V1. |
DISEASE ASSOCIATIONS AND DEFINITIONS
Atrial fibrillation is strongly associated with valvular pathologies such as mitral valve diseases and advanced aortic valve diseases as well as certain congenital heart diseases such as atrial septal defect. Those patients comprise a separate category with the risk profile and management different from nonvalvular atrial fibrillation patients. One should bear in mind that most studies in atrial fibrillation including rhythm versus rate control and stroke risk stratification were performed in patients with nonvalvular atrial fibrillation. Nonvalvular atrial fibrillation is commonly associated with hypertension, congestive heart failure, coronary artery disease, obesity, diabetes, obstructive sleep apnea, and primary cardiomyopathies such as hypertrophic cardiomyopathy. Atrial fibrillation can be a manifestation of sick sinus syndrome (tachycardia-bradycardia syndrome). Transient and reversible causes of atrial fibrillation include thyroid disease, acute pericarditis, pulmonary embolism, pulmonary diseases, heavy alcohol consumption, and cardiac surgery. In patients with no identified structural heart disease or predisposing condition, the term lone atrial fibrillation is sometimes used.
At our institution, a pathway for the management of atrial fibrillation has been developed and implemented.7




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
