Superior Sulcus Tumor
Presentation
A 65-year-old woman is referred to you with symptoms of cough and upper chest and shoulder pain. She denies fever, weight loss, and hemoptysis. She reports a 50-pack-per-year smoking history. On physical examination, blood pressure in the right arm is 120/80 mm Hg, there is no supraclavicular adenopathy, and the lung fields are clear to auscultation and percussion. The patient has a full range of motion of the right arm and hand. Blood chemistries are within normal limits.
Recommendation
The differential diagnosis for this includes pulmonary and mediastinal neoplasm. Chest wall abnormalities must also be considered. Inflammatory pulmonary disease should have associated systemic manifestations. A chest x-ray is an appropriate initial study.
▪ Chest X-rays
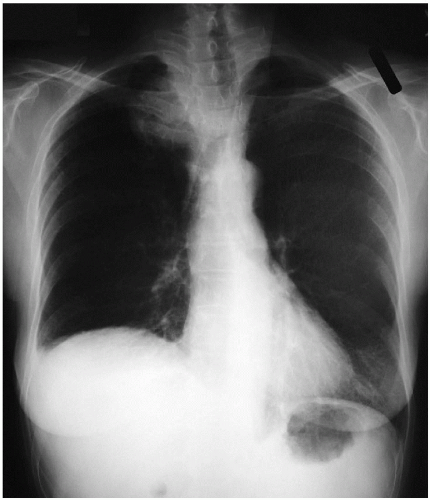 Figure 58-1 |
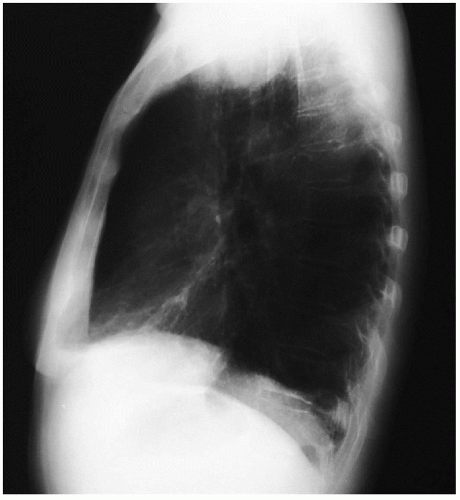 Figure 58-2 |
Chest X-ray Report
The chest x-rays reveal a mass in the upper right chest with possible compression of the trachea. The lateral chest x-ray shows the mass to be located anteriorly at the level of costosternal junction. Computed tomography (CT) scans are recommended for further anatomic delineation.
▪ CT Scans
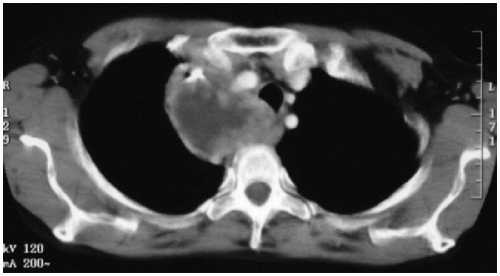 Figure 58-3 |
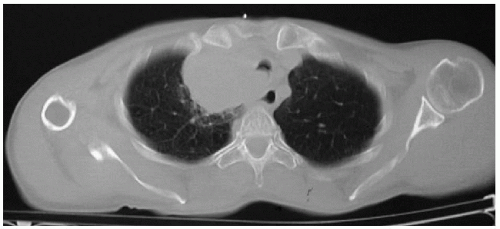 Figure 58-4 |
CT Scan Report
CT scans of the chest demonstrate a large anterior medial mass with central necrosis, which displaces the trachea to the left side and also is adjacent to the esophagus. Evaluation of all levels of the CT scans demonstrates compression and possible invasion of the subclavian artery and subclavian vein. No obvious enlarged mediastinal lymph nodes are seen.
Discussion
The radiologic appearance of the mass is suspicious for an anterosuperior sulcus lung cancer. Clinical staging is necessary to determine the histology of the mass and to define the extent of the cancer. Bronchoscopy with associated brushings and transbronchial biopsy can frequently fail to reveal a histologic diagnosis of cancer because of the more peripheral location of the lesion. Transthoracic needle aspiration biopsy provides a high incidence of histologic diagnosis. Mediastinoscopy is indicated to rule out metastasis to mediastinal lymph nodes because their positive involvement carries a very poor prognosis. Mediastinoscopy is recommended in all patients with superior sulcus tumors. The CT scans rule out the presence of neoplasm in the liver and adrenal glands. The patient has no central nervous system symptoms, and brain scan is not necessary. Magnetic resonance imaging (MRI) examination can be helpful in evaluating the brachial plexus when associated arm and hand symptoms are present. It can also define vascular involvement.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


