Cervical reconstruction of the subclavian artery is most commonly performed by a transposition onto or a bypass originating from the ipsilateral common carotid artery. There are advantages and disadvantages to both approaches, and the decision which to pursue often depends upon anatomic considerations and surgeon expertise. When performed by experienced surgeons, both procedures carry very low risk for complications.
Although the long-term patency rate for arterial transposition is virtually 100%, the long-term patency rates for a bypass are commonly reported to be 10% to 15% poorer than for transposition. On the other hand, arterial transpositions might not be possible when the vertebral artery takes off early from the subclavian artery or when the atherosclerotic process extends far distally beyond the vertebral origin. Another indication for carotid–subclavian bypass, as opposed to a transposition, would be in the patient with a patent internal mammary artery–coronary artery graft. With the use of a cervical bypass, the arterial clamps can be placed beyond the internal mammary artery to avoid myocardial ischemia.
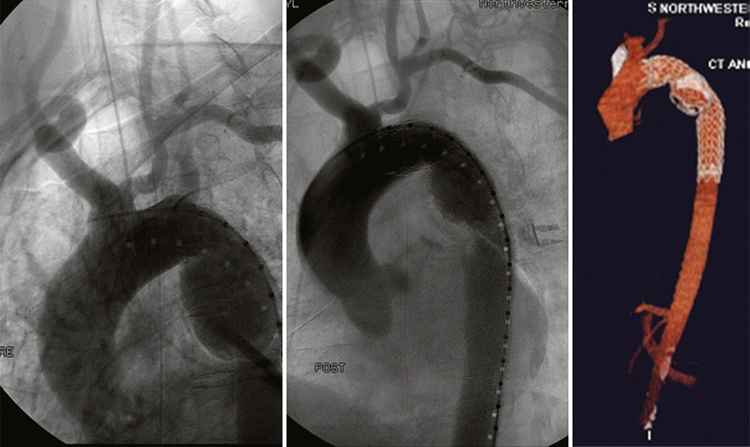
Cervical reconstruction by a transposition should be considered the surgical technique of choice for single proximal occlusive lesions involving the subclavian artery. In addition, with the advent of endovascular therapy for thoracic aortic disease, surgical manipulation of the supra-aortic trunks to prepare patients with thoracic and thoracoabdominal aortic aneurysms, dissections, or traumatic tears have become accepted and commonplace (Figure 1). Subclavian artery reconstruction is now commonly performed to preserve vertebral and left upper extremity flow while extending the proximal neck landing zone before deploying an endograft. Many consider an aggressive approach to pre-endograft revascularization of the left subclavian to optimize posterior brain, spinal cord, and upper extremity circulation to be imperative. Not only is preservation of the vertebral artery critical but it is equally important to mobilize and preserve the valuable internal mammary artery.
Transposition of the left subclavian clearly has a prominent role, and when there is a usable ipsilateral source vessel, an arterial transposition should be the first choice. When performed properly, transposition not only preserves arm, vertebral, and mammary flow, it also obviates the need for proximal subclavian ligation or transcatheter embolization of the vessel to prevent the development and persistence of a large retrograde type II endoleak, as would occur following bypass.
Arterial transpositions are completed through a short, transverse cervical incision above the clavicle. The incision is placed more medially than for bypass and is positioned to overlie the space between the two heads of the sternocleidomastoid muscle. The surgical dissection itself is carried out between the two heads of the sternocleidomastoid muscle. This is an important contradistinction to performing a bypass where the dissection is carried out lateral to the entire sternocleidomastoid muscle. For a transposition, after dividing the omohyoid muscle between ligatures or with electrocautery, the jugular vein is reflected laterally and the common carotid is reflected medially along with the vagus nerve.
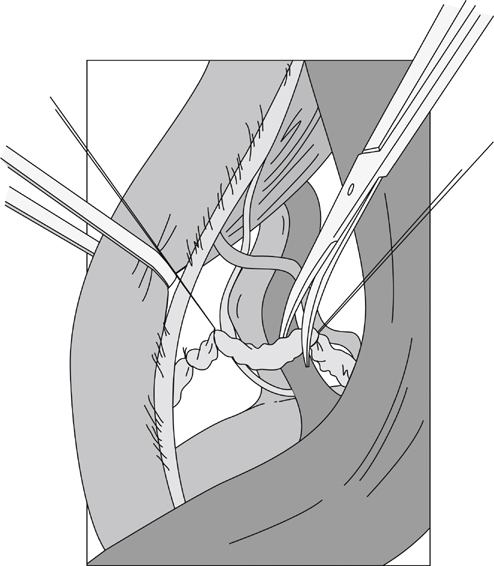
It is important to point out the difference in approach when compared to a bypass procedure. During a bypass, the jugular vein and vagus nerve are reflected medially to expose the common carotid beneath them. During a transposition, the medially reflected carotid is mobilized circumferentially with the dissection carried out deeply toward the mediastinum. On the left side, the thoracic duct and small identifiable lymphatics are identified, ligated, and divided (Figure 2). On the right, multiple cervical lymphatic channels must also be tied. After the vertebral vein is divided (Figure 3), the subclavian artery and its proximal branches can be identified behind the clavicle. If the vessel is patent, digital palpation can help with localization.
Only gold members can continue reading.
Log In or
Register to continue
Related

Stay updated, free articles. Join our Telegram channel