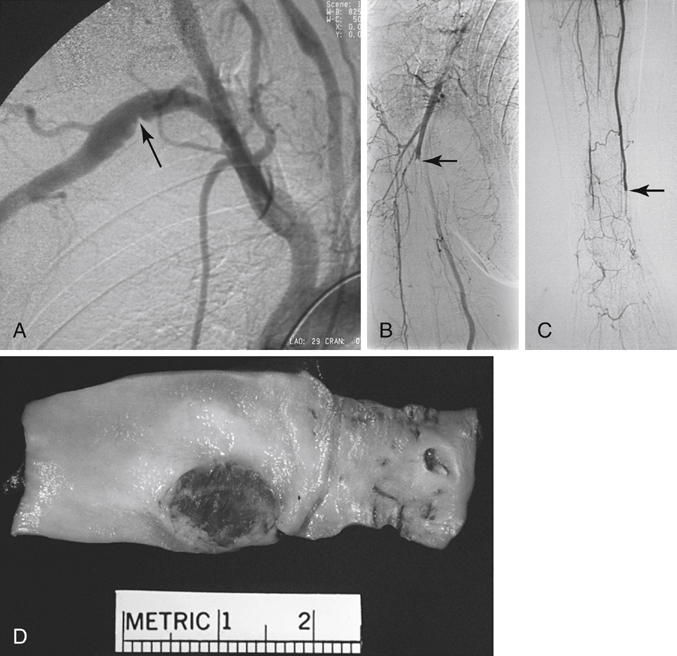
Nearly two thirds of patients are symptomatic at diagnosis, with neck and upper extremity pain from the compressive effect of the aneurysm the most common presentation (Table 1). Among our most recent 49 treated patients, symptoms occurred in 91% of patients with distal subclavian aneurysms, 61% with subclavian aneurysms, and 37% with proximal aneurysms. TABLE 1 Clinical Presentations in 49 Patients Treated for Subclavian Aneurysms between 1990 and 2005 Rupture and thromboembolism are the major complications of these aneurysms. The latter causes arm or hand ischemia or vertebral or carotid stroke by retrograde propagation and washout of thrombus. Chronic repetitive upper extremity or digital emboli from ulceration within a subclavian artery compressed by a cervical rib is a diagnosis that may be confused with collagen vascular disorders or inflammatory processes involving the small and medium-sized arteries of the extremity (Figure 1). Such presentations delay diagnosis. Nehler and colleagues reported the average time between onset of digital ischemia and diagnosis of the aneurysm to average 7 months, ranging as long as 36 months.
Subclavian and Axillary Artery Aneurysms
Subclavian Artery Aneurysms
Signs and Symptoms
Percentage
Symptoms in 27 Patients
Neck and upper extremity pain
93
Paresthesias
30
Cold upper extremity
30
Exertional fatigue
24
Paresis
10
Transient ischemic attack or stroke
10
Signs in 31 Patients
Pulsatile neck mass/bruit (includes 13 asymptomatic patients)
37
Decreased or absent pulses
33
Pallor
33
Neurologic deficit
10
Digital emboli
8
Other Signs
Distal thromboembolism in 7 patients
15
Cerebral embolism in 5 patients
10

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


