Spontaneous Pneumothorax
Presentation
A 42-year-old man presents to the emergency department complaining of sudden onset of right-sided chest pain accompanied by shortness of breath and cough. His symptoms started 3 days ago and have gradually worsened. The patient denies any history of trauma before the onset of symptoms. The physical examination is significant for mild distress, tachypnea, and absent breath sounds over the right chest with normal breath sounds over the left chest. The patient denies any similar history. His past medical history is negative. The patient says he presented to the emergency department because his symptoms have not improved.
▪ Chest X-rays
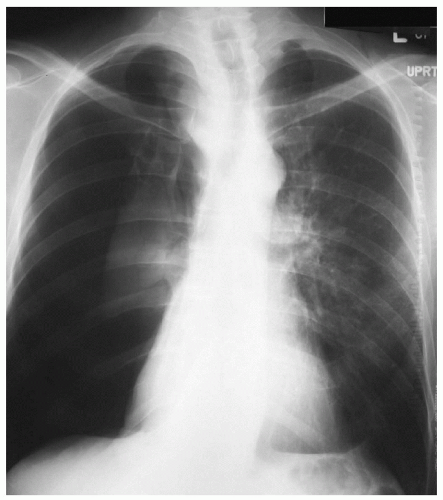 Figure 5-1 |
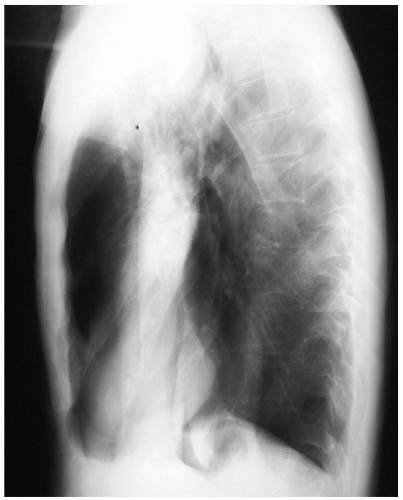 Figure 5-2 |
Chest X-ray Report
The posteroanterior and lateral chest x-rays reveal a right pneumothorax with complete collapse of the right lung. There is no evidence of mediastinal shift. The trachea is midline in position, with a depression of the right main-stem bronchus. The left lung is well inflated without any pathology. The heart size is normal.
Discussion
A spontaneous pneumothorax is one that occurs without any antecedent traumatic or iatrogenic cause. Spontaneous pneumothoraces can be categorized into primary or secondary types. A primary spontaneous pneumothorax occurs without any clinically apparent underlying lung disease known to promote a pneumothorax. The most common cause of primary spontaneous pneumothorax is an apical subpleural bleb. The typical patient is young, tall, and thin, and in late adolescence or early adulthood. The male-to-female ratio is 6:1. Clinical presentation may vary from asymptomatic (other than the initial chest pain episode) to tension pneumothorax with hemodynamic compromise or collapse. A secondary spontaneous pneumothorax occurs in lungs with underlying pathology that predisposes to a pneumothorax, such as cystic fibrosis, Marfan’s syndrome, metastatic osteosarcoma, Pneumocystis carinii, and asthma. Bullae are larger than blebs, usually larger than 1 cm. Rarely, a spontaneous pneumothorax may present with hemothorax due to disruption of vascular adhesions. The most common presentation, however, is without progression to tension pneumothorax. Symptoms also depend on the underlying baseline condition of the lungs, or of the remaining inflated lung. The plain chest x-ray is the standard diagnostic modality, preferably in the upright posteroanterior projection.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


