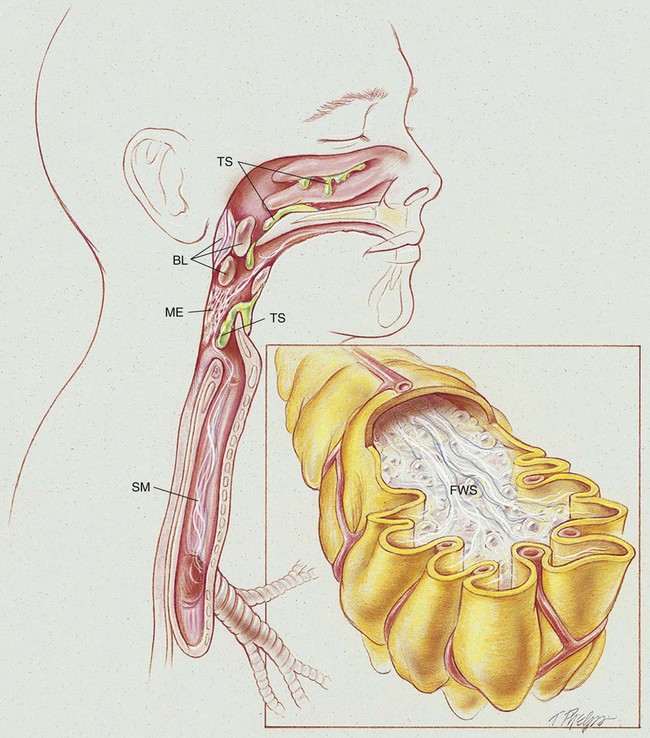
After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with smoke inhalation and thermal injuries. • Describe the causes of smoke inhalation and thermal injuries. • List the cardiopulmonary clinical manifestations associated with smoke inhalation and thermal injuries. • Describe the general management of smoke inhalation and thermal injuries. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. Even though thermal injury may occur with or without surface burns, the presence of facial burns is a classic predictor of thermal injury. Thermal injury to the upper airway results in blistering, mucosal edema, vascular congestion, epithelial sloughing, and accumulation of thick secretions. An acute upper airway obstruction (UAO) occurs in about 20% to 30% of hospitalized patients with thermal injury and is usually most marked in the supraglottic structures. When body surface burns require the rapid administration of resuscitative fluids, a UAO may develop rapidly (see Figure 41-1). Smoke inhalation also may cause acute respiratory distress syndrome (ARDS), noncardiogenic high-permeability pulmonary edema—commonly referred to in smoke inhalation cases as “leaky alveoli.” Noncardiogenic pulmonary edema also may be caused by overhydration resulting from overzealous fluid resuscitation (see insert panel in Figure 41-1). In severe cases, ARDS also may occur early in the course of the pathology. Thermal injury (upper airway—nasal cavity, oral cavity, and pharynx): Smoke inhalation injury (tracheobronchial tree and alveoli): • Inflammation of the tracheobronchial tree • Excessive bronchial secretions and mucous plugging • Decreased mucosal ciliary transport • Alveolar edema and frothy secretions (pulmonary edema) • COP (also called bronchiolitis obliterans organizing pneumonia [BOOP]) • Alveolar fibrosis, bronchial stenosis, bronchial polyps, bronchiolitis, and bronchiectasis (severe cases) Pneumonia (Chapter 15) and pulmonary embolism (Chapter 20) often complicate smoke inhalation injury. Smoke can result from either pyrolysis (smoldering in a low-oxygen environment) or combustion (burning, with visible flame, in an adequate-oxygen environment). Smoke is composed of a complex mixture of particulates, toxic gases, and vapors. The composition of smoke varies according to the chemical makeup of the material that is burning and the amount of oxygen being consumed by the fire. Table 41-1 lists some of the more common toxic substances produced by burning products that frequently are found in office, industrial, and residential buildings. TABLE 41-1 Toxic Substances and Sources Commonly Associated with Fire and Smoke Because the amount and severity of body surface burns play a major role in the patient’s risk of mortality and morbidity, an approximate estimate of the percentage of the body surface area burned is important. Table 41-2 lists the approximate percentage of surface area for various body regions of adults and infants. The severity and depth of burns usually are defined as follows: TABLE 41-2 The Approximate Percentage of Body Surface Area (BSA) for Various Body Regions of Adults and Infants First degree (minimal depth in skin): Superficial burn, damage limited to the outer layer of epidermis. This burn is characterized by reddened skin, tenderness, and pain. Blisters are not present. Healing time is about 6 to 10 days. The result of healing is normal skin. Second degree (superficial to deep thickness of skin): Burns in which damage extends through the epidermis and into the dermis but is not of sufficient extent to interfere with regeneration of epidermis. If secondary infection results, the damage from a second-degree burn may be equivalent to that of a third-degree burn. Blisters usually are present. Healing time is 7 to 21 days. The result of healing ranges from normal to a hairless and depigmented skin with a texture that is normal, pitted, flat, or shiny. Third degree (full thickness of skin including tissue beneath skin): Burns in which both epidermis and dermis are destroyed, with damage extending into underlying tissues. Tissue may be charred or coagulated. Healing may occur after 21 days or may never occur without skin grafting if the burned area is large. The resultant damage heals with hypertrophic scars (keloids) and chronic granulation. The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8), Alveolar Consolidation (see Figure 9-9), Increased Alveolar-Capillary Membrane Thickness (see Figure 9-10), Bronchospasm (see Figure 9-11), and Excessive Bronchial Secretions (see Figure 9-12)—the major anatomic alterations of the lungs associated with smoke inhalation and thermal injuries (see Figure 41-1). CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE
Smoke Inhalation and Thermal Injuries
Anatomic Alterations of the Lungs
Thermal Injury
Smoke Inhalation Injury
Early Stage (0 to 24 Hours after Inhalation)
Late Stage (5 or More Days after Inhalation)
Etiology and Epidemiology
Substance
Source
Aldehydes (acrolein, acetaldehyde, formaldehyde)
Wood, cotton, paper
Organic acids (acetic and formic acids)
Carbon monoxide, hydrogen chloride, phosgene
Polyvinylchloride (PVC)
Hydrogen cyanide, isocyanate
Polyurethanes
Hydrogen fluoride, hydrogen bromide
Fluorinated resins
Ammonia
Melamine resins
Oxides of nitrogen
Nitrocellulose film, fabrics
Benzene
Petroleum products
Carbon monoxide, carbon dioxide
Organic material
Sulfur dioxide
Sulfur-containing compounds
Hydrogen chloride
Fertilizer, textiles, rubber manufacturing
Chlorine
Swimming pool water
Ozone
Welding fumes
Hydrogen sulfide
Metal works, chemical manufacturing
Body Surface Burns
Anatomic Region
Percent of BSA in Adults
Percent of BSA in Infants
Entire head and neck
9
18
Each arm
9
9
Anterior trunk
18
18
Posterior trunk
18
18
Genitalia
1
1
Each leg
18
13.5
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Smoke Inhalation and Thermal Injuries
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Smoke Inhalation and Thermal Injuries