(1)
Department of General surgery, Fuwai Hospital, Beijing, China
19.1 General Considerations
Single ventricle is a congenital cardiac malformation in which both atria are connected to only one ventricle chamber by either two separate atrioventricular valves or a common AV. Usually, there are two ventricles. One is the large main chamber, whereas the other is always incomplete (rudimentary) and hypoplastic. However, there is only one chamber. The two great arteries originate from the single ventricle, and the interrelationship can be normal or transpositioned. Therefore, the single ventricle is supposed to be a group of integrated deformities involving the ventricle, atrioventricular valves, and great arteries. The single ventricle due to hypoplasia of ventricular septum is also known as the common ventricle.
19.2 Embryology
The embryonic mechanism of the single ventricle is the developmental abnormality of the ventricular segment of the primitive heart tube. The primitive heart tube is right loop shaped and bent normally. Lying in the bottom section of the heart tube is the primitive ventricle. Its right end develops into the sinus part of the RV and is linked to the atrioventricular canal. The muscular ventricular septum exists between the left and right sinus parts. The conus part rotates and straddles the two ventricles, forming the ventricular outflow tract. Thus, whether it is hypoplasia of the right end (sinus of right ventricle) or the left end (sinus of left ventricle) of the primitive ventricle, or muscular ventricular septum, it results in a single ventricle.
19.3 Typing
There are a variety of typing methods for single ventricle. From the practical point of surgery, the following characteristics should be emphasized:
1.
The main chamber of the single ventricle is equivalent to the left or right ventricle.
2.
Either a common AV valve or two separate atrioventricular valves.
3.
Conus structure under the valve of the great arteries or not.
4.
Rudimentary ventricular septum or not.
5.
Positional relationship between the great arteries.
6.
Pulmonary stenosis or atresia or not.
7.
Other combined deformities.
19.4 Hemodynamics
The hemodynamics can be analyzed using the “imaginary blood flow direction.” If the blood flows from the LA to the AV through the arterial atrioventricular valve, it would be assumed to be the arterial blood line; then, the blood flow from the RA to the pulmonary valve through the venous atrioventricular valve would be the venous blood line. If these two lines are parallel to each other, the two blood flows could be separated by an artificial ventricular septum. However, if these two lines cross in the heart, the malformation could not be repaired by artificial ventricular septum.
19.5 Surgical Management
Palliative surgery is the main therapy for the single ventricle. The shunt operation, such as the vena cava-pulmonary artery shunt or the bidirectional Glenn operation, is indicated for less pulmonary blood. The pulmonary banding is indicated for more pulmonary blood. The ideal separation operation is to divide the single ventricle into left and right ventricles; however, that approach cannot be implemented in most cases because of the swing of the artificial ventricular septum and the abnormality of transduction bundles.
19.6 Specimen Demonstrations
19.6.1 Single Ventricle, Double-Inlet Ventricle
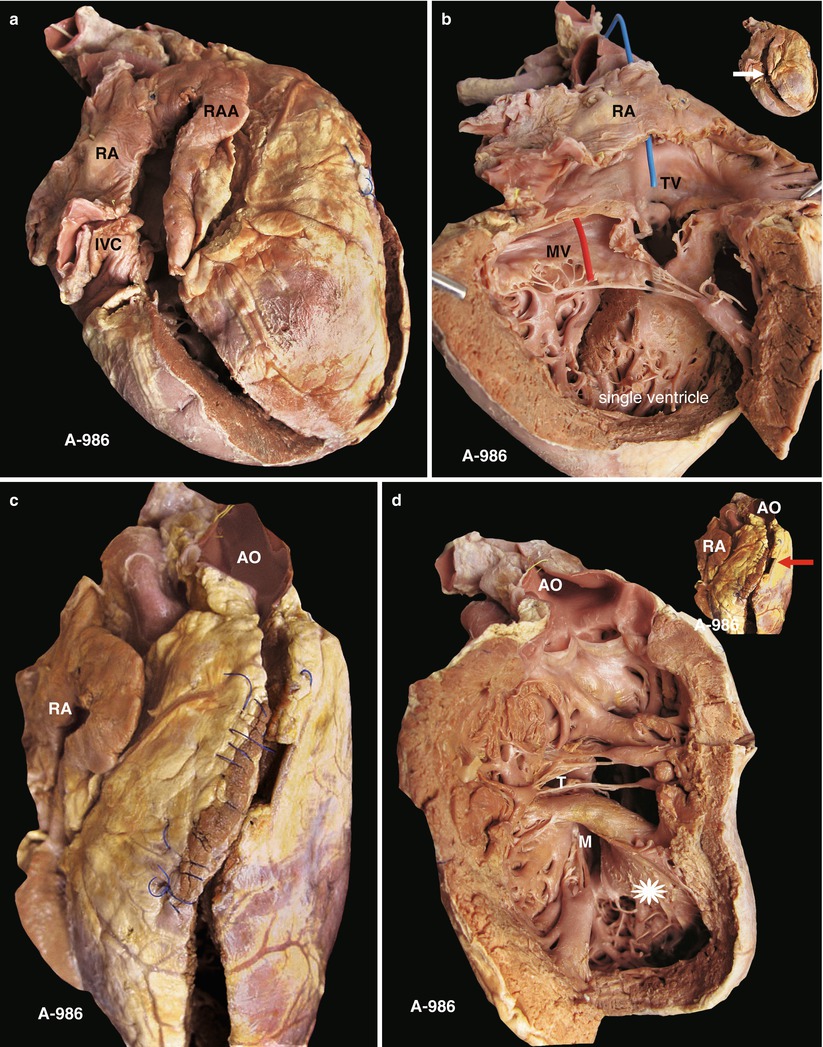
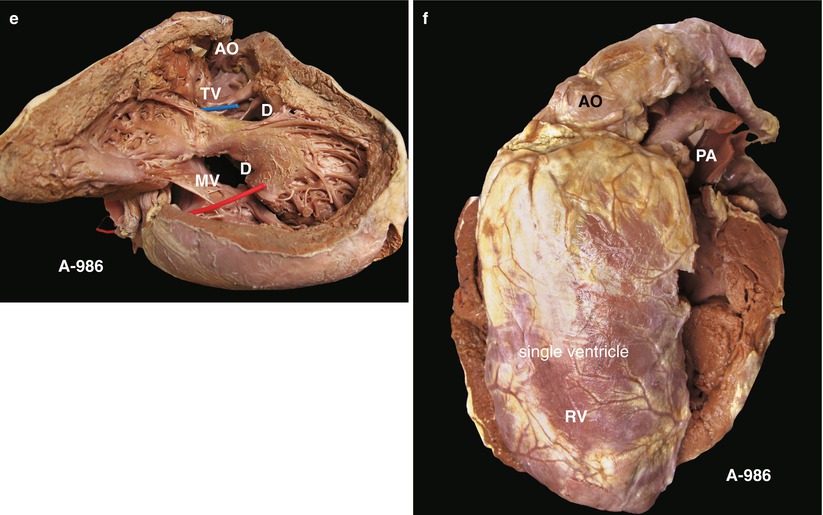
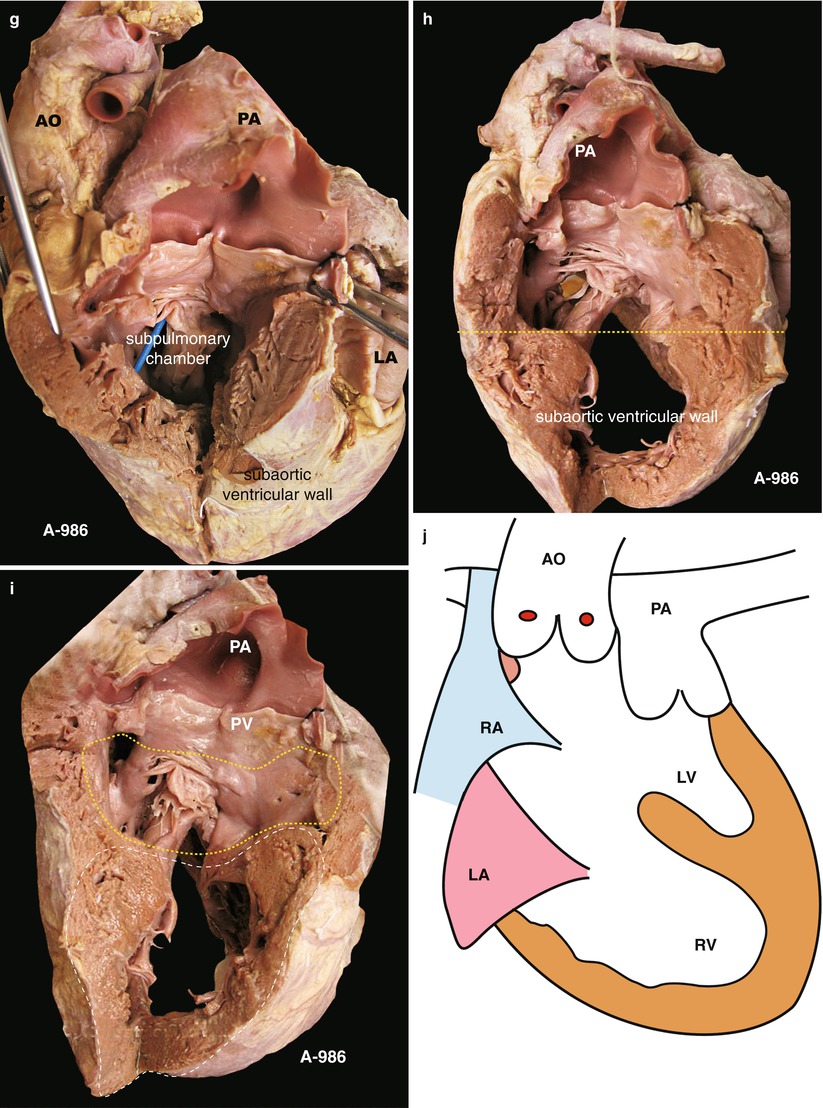
Fig. 19.1
(a) Specimen 986. The right-sided view of the double-inlet ventricle and the conus under the aortic valve. The RA, RAA, and IVC all are on the right. The right-sided ventricle is the subaortic valve chamber, which can be interpreted as the main chamber of the single ventricle. IVC inferior vena cava, RA right atrium, RAA right atrial appendage. (b) Specimen 986. Inflow tract of right-sided ventricle. The blue and red indicate the blood flow of the right or left atria, respectively. The MV and TV are open to the same huge ventricular chamber, which is the main chamber of the single ventricle. The arrow in the upper right corner indicates the incision site. MV mitral valve, TV tricuspid valve. (c) Specimen 986. Subaortic ventricular incision. The sutures of the operative incision are shown. The anterior aorta and inferior PV indicate the abnormal position relationship of the great arteries. AO aorta. (d) Specimen 986. Sufficient exposure of the ventricular chamber under the aortic valve, which is the main chamber of a single ventricle. Trabecular area (asterisk) is the free wall of the ventricle but not of the ventricular septum. The TV and AV are separated by the conus muscle. The ventricular septum nearly disappears; remaining are the subaortic conus muscle, the bundles of thick muscle, and the apical trabecular muscle. AV aortic valve, TV tricuspid valve. (e) Specimen 986. The thick muscle bundles and abundant trabecular muscle in accord with morphological right ventricle structure. “D” indicates the huge VSD. The blue and red indicate the blood of both the TV and MV inflow to the subaortic ventricular chamber. MV mitral valve, TV tricuspid valve, VSD ventricular septal defect. (f) Specimen 986. Left-side view of the positional relationship of the great arteries. The aorta and main pulmonary artery originate from the same ventricle. The former is located anteriorly and the latter inferiorly. This positional relationship belongs to transposition of the great arteries. (g) Specimen 986. A small ventricle under the pulmonary valve, which could be interpreted as a subpulmonary chamber. Actually, it belongs to the same ventricular chamber as does the subaortic chamber. No ventricular septum exists between them, and only bundles of free muscle are found. Continuous fiber exists between the pulmonary valve and the TV. The blue was inserted from the TV into the subpulmonary chamber. The inferior wall is the free wall of the contralateral main ventricular chamber. TV tricuspid valve. (h) Specimen 986. Range of ventricular chamber. Above the dotted line is the subpulmonary chamber, which is hypoplastic. Below the line is the right side of the subaortic chamber. (i) Specimen 986. The comparison of two ventricular chambers. The white and yellow dotted lines indicate the subaortic chamber and the subpulmonary chamber, respectively. PA pulmonary artery, PV pulmonary valve. (j) Specimen 986. Schematic diagram of double-inlet ventricle. LV indicates the residual cavity of the morphological LV, whereas RV indicates the morphological RV. There is no ventricular septum. The blue and red lines indicate the tricuspid and mitral valves, respectively. AO aorta, LA left atrium, LV left ventricle, PA pulmonary artery, RA right atrium, RV right ventricle
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


