Chapter 11 Silicone Stent Insertion for Focal Crescent–Type Tracheomalacia in a Patient with Sarcoidosis

Case Description
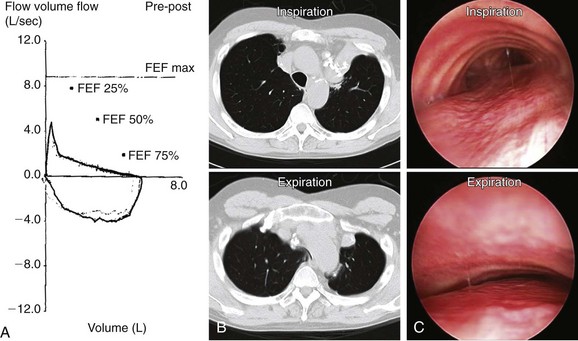
A 62-year-old man with a history of pulmonary sarcoidosis diagnosed 10 years earlier presented with chronic cough and inability to clear secretions. He described his cough as “seal barking.” He had also noted increasing dyspnea with normal physical activities. For the past month, his primary care physician had treated him with short- and long-acting bronchodilators, as well as inhaled and systemic steroids (prednisone 20 mg/day) for suspected adult-onset asthma. He was a nonsmoker, worked as an electrician, and had a history of hypertension and supraventricular tachycardia controlled by diltiazem. Electrocardiogram (ECG) and two-dimensional (2D) echocardiogram were unremarkable. Pulmonary function testing (PFT) revealed moderate obstructive ventilatory impairment without improvement after bronchodilators. Flow volume loop (FVL) showed an airway collapse pattern on the expiratory curve (Figure 11-1). Paired inspiratory/expiratory dynamic computed tomography showed bilateral upper lobe fibrosis, tracheomegaly, and localized narrowing of the lower trachea during dynamic expiration (see Figure 11-1). Flexible bronchoscopy revealed fibrotic closure of the right and left upper lobar bronchi and complete expiratory collapse of the anterior cartilaginous structures in the lower trachea, giving the airway lumen the shape of a crescent (see Figure 11-1).
Case Resolution
Initial Evaluations
Physical Examination, Complementary Tests, and Functional Status Assessment
This patient presented with dyspnea, cough, and mucus retention. These nonspecific symptoms of pulmonary disorders are seen primarily in patients suffering from asthma, chronic obstructive pulmonary disorder (COPD), or bronchiectasis. His cough, however, was described as “seal barking.” This pattern is suggestive of expiratory central airway collapse (ECAC) and presumably is caused by vibration of the floppy membranous posterior wall against the anterior airway wall during expiration.1 As in our patient, symptoms are usually refractory to corticosteroids and bronchodilators.2 In addition, patients with ECAC may have recurrent bronchitis, pneumonia, and even respiratory failure.3 Some patients experience cough-syncope, presumably as a result of a significant rise in intrathoracic pressure and a sudden drop in venous return and cardiac output4 during violent coughing episodes.
Spirometry showed obstructive ventilatory impairment. In ECAC, spirometry usually demonstrates obstruction that is proportionate to the severity of the disease.5 The expiratory FVL seen in this patient suggested compression of the central airways (see Figure 11-1). This “airway collapse” pattern occurs when maximal flow is quickly reached after expiration of a small volume of air. Following maximal flow, a large fall in flow occurs, although only a small volume is exhaled. Subsequently, the flow rate falls very little during the remainder of expiration. This phase is responsible for the long plateau seen on the FVL (see Figure 11-1).6 However, the FVL is neither sensitive nor specific; it can be seen in almost 40% of patients with severe COPD.7 Flow oscillations on the FVL have also been described. These take on a sawtooth appearance, defined as a reproducible sequence of alternating decelerations and accelerations of flow. This pattern is nonspecific because it can be seen in patients with obstructive sleep apnea, structural or functional disorders of the upper airway, and neuromuscular diseases.8 Lack of clinical and spirometric improvement after bronchodilator administration might be explained by the effects of bronchodilators on central airways. Bronchodilators cause smooth muscle relaxation, further decreasing tracheobronchial wall stiffness and worsening airway obstruction. Bronchodilators increase airway wall compliance. The resulting increased airway compressibility will cause the choke point to be localized to a point closer to the thoracic outlet. The increased length of the upstream segment (from the alveoli to the choke point) and the decreased cross-sectional area at the choke point offset any advantages gained by bronchodilator-induced caliber increase in upstream airways with respect to maximal expiratory flow.9 In fact, although this effect has not been studied in adults, a dramatic fall in peak flow in response to bronchodilators has been described in pediatric cases of tracheobronchomalacia (TBM).10*
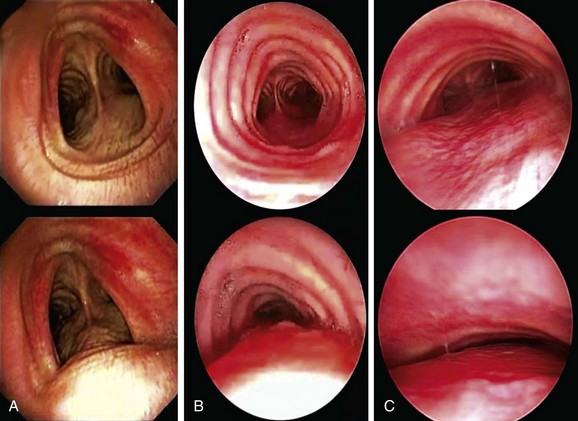
In our patient, a diagnosis of expiratory central airway collapse was made bronchoscopically and on paired dynamic inspiratory/expiratory computed tomography (CT) scanning. Because of the obvious weakness of the lower anterior tracheal cartilaginous wall, this patient had focal crescent tracheomalacia.11 The disorder was characterized by a severe (100%) degree of airway narrowing. During dynamic (functional) bronchoscopy, the airways were visualized by moving the patient into supine, upright, and lateral decubitus positions during spontaneous breathing, as well as during cough, forced expiration, and deep inspiration. During these bronchoscopic assessments, changes in airway lumen can be measured and the extent of collapse noted, and narrowing can be classified as being of the crescent, saber-sheath, or circumferential type. Regions of cartilaginous weakness (tracheomalacia) can be differentiated from areas of excessive dynamic airway collapse (EDAC) or normal physiologic dynamic airway collapse (DAC) (Figure 11-2).
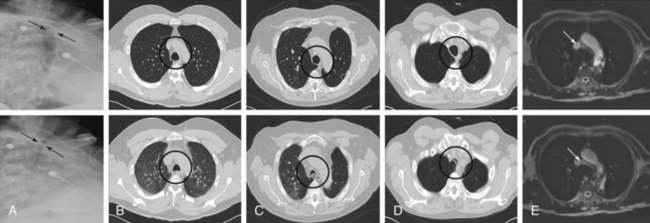
Among radiologic studies, fluoroscopy was used to diagnose tracheomalacia in the past. During fluoroscopy, one can visualize the airway collapse, but it is difficult to appreciate whether it is due to softening of the cartilage or to excessive bulging of the posterior membrane (Figure 11-3).12 Today, with the use of dynamic CT, one more easily distinguishes cartilaginous from posterior wall collapse (see Figure 11-3). Results from studies show that dynamic CT correlates well with bronchoscopy findings,13 offers excellent display of anatomic details of the airway and adjacent structures,14 and allows objective interpretation and quantitative measurements of the degree of airway wall collapse before and after airway splinting interventions.14,15 Dynamic magnetic resonance imaging (MRI) has been insufficiently studied, but small case series support its use for quantifying the degree of airway collapse16 (see Figure 11-3). Its main advantage over CT is that radiation is avoided and contrast materials used are not nephrotoxic.
We quantified this patient’s functional impairment on the basis of World Health Organization (WHO) functional class criteria.17 He had WHO class II functional impairment defined as mild limitation of physical activity without discomfort at rest, but with normal physical activity causing increased symptoms.18 The use of other dyspnea or quality of life (QOL) instruments (St. George’s Respiratory Questionnaire [SGRQ], American Thoracic Society [ATS] Dyspnea Scale, Baseline Dyspnea Index [BDI]/Transitional Dyspnea Index [TDI], Karnofsky Performance Scale [KPS], and a 6-minute walk test [6MWT]) in these patients to objectively determine response to interventions has been studied.19
Comorbidities
The patient had controlled cardiac arrhythmia and no evidence of systolic or diastolic dysfunction on 2D echocardiogram. Although moderate obstructive ventilatory impairment was noted, clinical evaluation and the 2D echocardiogram showed no evidence of pulmonary hypertension, which might prompt hemodynamic instability in case of general anesthesia.20
The patient had been on prednisone 20 mg/day for 4 weeks. Traditionally, any patient who has received the equivalent of 15 mg/day of prednisone for longer than 3 weeks should be suspected of having hypothalamic-adrenal axis suppression.21 As a general rule, any patient who has received glucocorticoids in doses equivalent to at least 20 mg/day of prednisone for longer than 5 days is at risk for hypothalamic-pituitary-adrenal (HPA) axis suppression.22 Furthermore, this patient had been on high-dose inhaled fluticasone (440 mcg twice daily) for several years. The development of adrenal suppression from inhaled steroids is known to be related to dose, duration of therapy, and use of a potent agent (such as fluticasone).23
Support System
The patient is married, but his wife suffers from severe COPD and is on continuous home oxygen supplementation. He is her caregiver. Investigators have found that informal caregivers (defined as untrained and unpaid persons who provide care to an ill person) have needs that go largely unmet, and that they usually receive insufficient help from services with regard to daily physical caring and emotional issues, as well as regarding information about available health and social services. Caring for a patient with dyspnea is particularly challenging and is most difficult to cope with.24
Patient Preferences and Expectations
Similar to other people caring for patients with dyspnea, this patient expressed uncertainty about the future and feared there would come a time when he could no longer help his spouse, or that helping her would be done at the expense of his own health. Active participation and availability of health care professionals are needed to assist informal caregivers with coping strategies they are already using and to address future challenges. Greater involvement of health care professionals leads to sharing of information and advice, thereby enhancing the informal caregiver’s competence, especially in managing difficult symptoms such as dyspnea.24 This patient was particularly motivated to improve his own symptoms so that he could maintain and improve his caregiving role for his wife. He had clearly expressed his willingness for treatment and was ready to consider all available treatment options, including noninvasive positive-pressure ventilation, airway stent insertion, and open surgical resection if necessary.
Procedural Strategies
Indications
Focal Tracheomalacia Resulting in Functional Impairment
The treatment of severe malacia often involves the use of minimally invasive or open surgical procedures.25,26 The exact degree of expiratory airway narrowing responsible for symptoms and requiring intervention remains unknown. Many investigators use 50% or greater reduction in airway caliber between inspiration and expiration to identify abnormal central airway collapse on dynamic CT or bronchoscopy.27–29 This criterion, however, is applied during coughing or forced exhalation, and its use may lead to false-positive results: 78% of normal individuals exceed the current diagnostic criterion for tracheomalacia in the upper and/or lower trachea.30 Furthermore, patients with other airway disorders such as bronchiolitis, COPD, or cystic fibrosis have peripheral airway obstruction, and the expiratory airway collapse seen in the central airways represents normal physiology.31–33 Indeed, during flow-limited breathing, the central airways become severely compressed, particularly during forced expiration and cough—maneuvers often used in diagnosing this entity on dynamic imaging studies. The Starling resistor model* shows that the pressure drop occurs across a very short length of airway, and that proximal airway (downstream from the choke point, mouth ward) resistance should not affect airflow. Pressure catheter measurements demonstrate this flow-limiting choke point and lack of further pressure drop in airways between the mouth and the flow-limiting segment.34 Because the choke point in adult humans is often located at the level of the lobar bronchi and is even more peripheral in patients with COPD,35 central airway collapsibility should not impede airflow.32
Our patient had severe (100%) collapse, resulting not just in exertional dyspnea but also in refractory cough and inability to raise secretions. For these reasons, after taking into account the patient’s goals of care, we elected to proceed with rigid bronchoscopy under general anesthesia to place an indwelling silicone stent that would splint open the lower trachea. Our goal was to improve airway lumen patency to less than 50% collapse during exhalation, which, by convention, is currently considered by most investigators to be within normal limits.17
Expected Results
In the short term (up to 10 to 14 days), airway stabilization with silicone stents in patients with various forms of expiratory central airway collapse was shown to improve respiratory symptoms, quality of life, and functional status.18,19 In one large study evaluating stent insertion for this disease, 45 of 58 patients (77%) reported symptomatic improvement; quality of life scores improved in 19 of 27 patients (70%) (P = .002), dyspnea scores improved in 22 of 24 patients (91%) (P = .001), and functional status scores improved in 18 of 26 patients (70%) (P = .002).19
Team Experience
Silicone stent insertion requires rigid bronchoscopy—a skill possessed by a minority of pulmonologists.36 Even for those who have undergone training, the technique of gentle, atraumatic rigid intubation and stent insertion is one that is gradually perfected over time.
Therapeutic Alternatives for Restoring Airway Patency
These include conservative, minimally invasive, and open surgical therapies.
• Continuous positive airway pressure (CPAP): Excessive airway narrowing and the resulting turbulent flow result in increased airway resistance, which requires greater transpulmonary pressures to maintain expiratory airflow. This will increase the work of breathing and will result in dyspnea. Adjunctive noninvasive positive-pressure ventilation decreases pulmonary resistance and can be used to maintain airway patency, facilitate secretion drainage, and improve expiratory flow. Small studies have showed that the addition of nasal CPAP improves spirometry values, sputum production, atelectasis, and exercise tolerance, but its long-term efficiency has not been clearly demonstrated.37,38
• Metal stent insertion: This approach has been used in the past with variable success.11 Advantages include placement by flexible bronchoscopy, dynamic expansion, and preservation of airway mucociliary function with uncovered stents. In some studies, however, metal stents had to be removed because of stent failure, or because of stent-related complications. Stent fracture and fatal hemorrhage from perforation, for example, have been reported.39 The Food and Drug Administration (FDA) recommends against the use of metallic stents for histologically benign forms of airway obstruction, as in the case described herein.40
• Open surgical interventions: Airway splinting has been used to consolidate and reshape the airway wall. Before an open surgical intervention is proposed, a stent trial has been recommended to identify those patients who are likely to benefit from surgery over the long term. Among surgical interventions, membranous tracheoplasty seems to provide a favorable outcome in uncontrolled studies. This procedure reinforces the membranous portion of the trachea in severe diffuse expiratory central airway collapse.41,42 However, our patient had mild functional impairment and focal disease limited to the lower trachea, probably warranting a more conservative approach.
• Tracheostomy: This technique may be used to splint the malacic airway and provide invasive ventilatory support if necessary; because it can be complicated by secondary tracheomalacia and stenosis at the stoma site, it should not be considered a first-line treatment in elective cases. In our case, the malacic segment would not have been bypassed by tracheostomy because it was localized in the lower trachea.
• Tracheal resection has been proposed for focal tracheomalacia with good outcome and low mortality in experienced centers.43 This procedure, however, has been performed for post-tracheostomy–related malacia, not for lesions localized in the lower trachea.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


