Preliminary speckle-tracking echocardiographic studies show that patients with single ventricles (SVs) have significantly decreased twisting and dyssynchrony of twisting. This could be related to abnormal cardiac looping, which leads to hearts that lack helical fiber patterns. The aim of this study was to analyze gradient cine magnetic resonance imaging (MRI) using Velocity Vector Imaging to assess cardiac mechanics. Subjects were 38 patients (aged 8 to 37 years) with SVs of left ventricular (n = 30) and indeterminate (n = 8) type who underwent cardiac MRI. Controls were 14 normal children and adults. Gradient cine MRI sequences close to the apex were subjected to a Velocity Vector Imaging analysis program adapted for MRI. In the control group, mean circumferential strain was −18.02 ± 7.31%, mean dispersion of peak circumferential strain was 44.23 ± 37.14 ms, and average rotation was −7.7 ± 1.38°. The rotation values were negative, or counterclockwise. In patients with SVs, mean circumferential strain was −8.87 ± 7.30%, mean dispersion of peak circumferential strain was 181.55 ± 76.07 ms, and average rotation was −2.6 ± 1.24° (p <0.001). Mean dispersion of the peak of rotation in the control group was 39.6 ± 22.8 ms, compared to 166.5 ± 72.4 ms in patients with SVs. In conclusion, this study showed a dramatic decrease in apical rotation and circumferential strain in the SV group compared to the control group. Strain and rotation mechanics at the apex in patients with SVs showed marked dyssynchrony.
Speckle-tracking analysis has shown, in a preliminary study from our laboratory published in abstract form, that echocardiographic images of single ventricles (SVs) show decreased rotation and dyssynchrony of twist. The aim of this study was to assess the strain and rotational deformation in patients with SVs of left ventricular or indeterminate type compared to normal hearts using a speckle-tracking program, Velocity Vector Imaging (VVI; Siemens Medical Solutions USA, Inc., Mountain View, California), applied to magnetic resonance imaging (MRI) cines. We were the first to validate the VVI program applied to MRI in normal hearts. This is the first report of this technique being applied to gradient magnetic resonance images of patients with SVs.
Methods
Our study was a multicenter study and included MRI studies obtained at Oregon Health & Science University (Portland, Oregon), The Royal Brompton National Heart and Lung Hospital (London, United Kingdom), Texas Children’s Hospital (Houston, Texas), and the University of Washington (Seattle, Washington). We included patients with SVs that were of left ventricular or indeterminate type who had undergone cavopulmonary anastomosis procedures. Our controls were patients with normal hearts. The institutional review board at Oregon Health & Science University approved the study. For studies sent to us from outside institutions, patients’ identifications had been replaced by numeric codes.
The speckle-tracking program, VVI, was applied to the magnetic resonance images. VVI is commercially available for the analysis of 2-dimensional echocardiographic images, but not for magnetic resonance images. Here, the VVI analysis program used was adapted for MRI mechanical function. All magnetic resonance images were acquired using an electrocardiographically gated 1.5- or 3.0-T magnet. Depending on the center at which the images were acquired, the images were obtained with Intera 3T (Philips Medical Systems, Andover, Massachusetts) or GE Healthcare (Milwaukee, Wisconsin) systems. At 1.5 T, the cine sequences were run in steady-state free precession mode, while at 3 T, the images were acquired in conventional gradient-echo mode, without steady-state free procession mode. The gradient-echo cine loop images were converted from Digital Imaging and Communications in Medicine to Audio Video Interleave format and were analyzed using the VVI myocardial method.
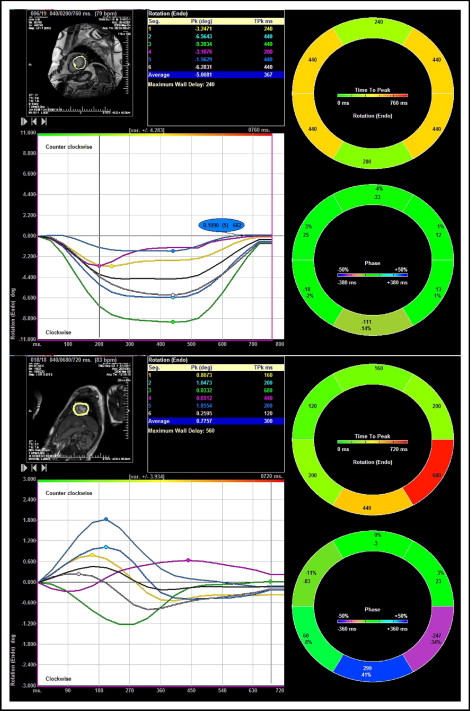
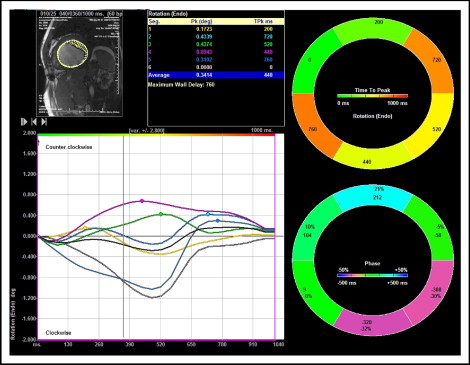
Short-axis MRI sequences were used. Images were acquired at frame rates of 15 to 25 frames/s. VVI was applied to gradient cine MRI sequences close to the apex for the SV and control groups. The endocardial borders of the SVs in the subjects and the left ventricles of the controls were traced manually in end-diastole ( Figures 1 and 2 ). VVI parameters were generated for 6 radial segments, as is standard for VVI, of the ventricles. These parameters included circumferential strain, rotation, and time to peak for both. The average of each parameter was compared between the SV and control groups.
Results
Cardiac magnetic resonance images of SVs after cavopulmonary anastomosis were analyzed. Thirty-eight children and adults made up this group, aged 8 to 37 years (mean 18). The control group was composed of 14 patients (mean age 22 years). The percentages of men in the SV and control groups were 60% and 50%, respectively.
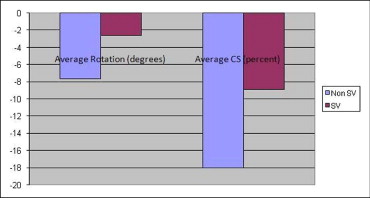
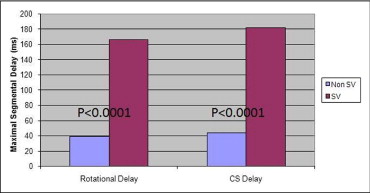
MRI short-axis cines were analyzed by VVI near the apical level. For the control group, mean circumferential strain was −18.0 ± 7.3%, whereas for the SV group, mean circumferential strain was reduced to −8.9 ± 7.3% (p <0.0001; Figure 3 ). Mean dispersion of peak circumferential strain was 44.2 ± 37.1 ms in the control group and 181.6 ± 76.1 ms in the SV group ( Figure 4 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


