Data on relational and sexuality issues in adult patients with congenital heart disease (CHD) are scarce. The present study aimed to evaluate relational and sexual behaviors, satisfaction, and functioning in a representative sample of patients with CHD and their partners. In addition, we aimed to evaluate the relation between sexuality parameters and quality of life. Relational and sexuality issues were assessed using a sexuality questionnaire in 133 patients (52% men, 37 ± 13 years old) with CHD (43 with coarctation of the aorta, 42 with transposition of great arteries, 36 with Marfan syndrome, and 12 with Eisenmenger syndrome), and 74 partners. Quality of life was assessed using the Dutch translation of the Medical Outcomes Study Short Form 36-Item Health Survey. Data were compared to an age- and gender-matched control group (n = 3,642). Seventy-one percent of patients with CHD were involved in a relationship, which was significantly less compared to controls (79%, p <0.05). Nonetheless, patients perceived their relationship as more satisfactory compared to controls (p <0.05). Overall, sexual satisfaction was equal in patients compared to controls, although they perceived lower body esteem (p <0.001), decreased sexual esteem (p <0.05), and more distress during sex (p <0.001). Patients reported no more erectile and lubrication problems compared to partners and to controls. We found significant associations between most relational and sexual parameters and quality of life. In conclusion, many aspects of sexuality are affected in adult patients with CHD, whereas their partners remain relatively unaffected. Moreover, sexuality is an important aspect of quality of life in these patients. We advise physicians to be receptive to discuss sexuality issues and provide patients with adequate therapy.
Sexuality is considered an important aspect of quality of life in patients with acquired heart disease and is receiving increased attention. It is known that patients with acquired heart failure have loss in sexual interest, decreased sexual frequency, decrease of sexual satisfaction, and increased incidence of sexual dysfunction. Although changes in patients’ sexuality seem to have no negative influence on marital relationships, partners are known to have distress during sexual contact and a decrease in frequency of sexual contact. Sexuality in patients with congenital heart disease (CHD) could well be equally affected, because their physical condition is often deteriorated, complications are numerous, and the use of medication is high. Nonetheless, knowledge on sexuality in adult patients with CHD remains sparse. Only few studies have been performed on the subject, focusing primarily on young men or on reproductive issues in women with CHD. To overcome this hiatus in current knowledge, the present study aimed to evaluate relational and sexual behavior and satisfaction and sexual functioning in a representative sample of adult patients with CHD and their partners. In addition, we evaluated the influence of relational and sexuality issues on these patients’ quality of life.
Methods
Adult patients with CHD were derived from the CONgenital COR vitia (CONCOR) registry, the Dutch national registry of adult patients with CHD. Two hundred thirty-one patients (70 patients with Marfan syndrome, 69 patients with coarctation of the aorta, 67 patients with transposition of great arteries, and 25 patients with Eisenmenger syndrome) were eligible to participate in the study and were contacted by telephone (from November 2008 to May 2009) to request their participation. Patients with partners were asked to request their current partner’s participation. An age- and gender-matched control group (n = 3,642) was used to compare patients and their partners to the Dutch population. The control group was recruited by the Rutgers Nisso Group, the Dutch Expert Center on Sexuality (Utrecht, The Netherlands), using the Internet panel Euroclix (>200,000 members). Recruitment was performed from November 2005 to February 2006. The first 2,000 subjects were randomly recruited from this panel, after which specific groups of subjects were requested to participate in the study to obtain a representative sample from the Dutch population.
The study complied with the Declaration of Helsinki and was approved by the ethics committees of all participating tertiary referral centers.
Patients’ and their partners’ relational and sexual behavior, satisfaction, and functioning were evaluated using a 169-item sexuality questionnaire, which was developed for this study in collaboration with the Rutgers Nisso Group. The questionnaire consisted of 5 domains ( Appendix 1 ), online only. In summary, “subjective health perception” focused on patients’ current health perception. “Relational satisfaction” contained questions on marital status and satisfaction with a current relationship, whereas “sexual satisfaction” contained questions on sexual behavior and sexual perception. “Sexual functioning” included gender-specific sexual dysfunction, and “sexuality and cardiac condition” focused on heart disease-related emotional and physical problems in relation to sexuality. For the latter domain, data were not obtained from the general population. All subjective sexuality scores ranged from 1 to 5, except sexual distress, which was scored 1 to 4, with higher scores representing a more positive sexual attitude. In addition, patients were asked whether they were interested in receiving additional information on sexuality and CHD.
Health-related quality of life was assessed with the Dutch translation of the Medical Outcomes Study Short Form 36-Item Health Survey (SF-36), which consists of 36 questions on 8 domains (physical functioning, role functioning physical, bodily pain, general health perception, vitality, social functioning, role functioning emotional, and mental health). Scores range from 0 to 100, with higher scores representing better quality of life. The 8 domains were combined into 2 higher-ordered clusters, the physical component summary (PCS) and the mental component summary (MCS). Patients’ SF-36 scores were compared to published age- and gender-matched norms from a Dutch reference population.
For statistical analyses SPSS 16.0 for Windows (SPSS, Inc., Chicago, Illinois) was used. Statistical significance was set at a p value <0.05. Descriptive data are presented as mean ± SD if normally distributed or as median with range, as appropriate. The 8 dimensions of the SF-36 scores were converted to standard scores based on scores of an age- and gender-matched representative reference sample of the Dutch population. A standard score indicates how many SDs the observed SF-36 score decreases below or above the score from the reference population. Consequently, the score of the reference population is set at 0. Linear regression analysis was used to identify and estimate risk factors for decreased relational and sexual parameters. Comparison of discrete variables was performed using chi-square or Fisher’s exact test. Comparison of continuous variables between 2 groups was performed using unpaired Student’s t test or Mann-Whitney test if data were not normally distributed, and comparison of continuous variables among ≥3 groups was performed using analysis of variance or Kruskal-Wallis test and post hoc tests with Bonferroni correction.
Results
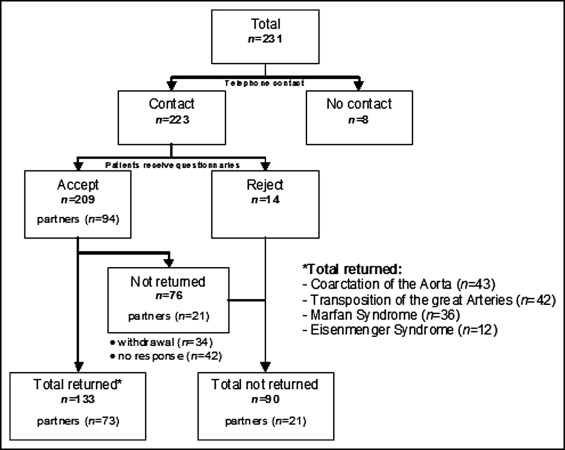
Of 231 eligible patients, 223 (97%) could be reached by telephone, of whom 209 (90%) agreed to participate. In total 133 patients returned their questionnaires, as did 73 partners ( Figure 1 ). There were no statistically significant differences in cardiac condition, gender, or age between patients who did and those who did not return the questionnaire or between patients and their partners ( Table 1 ). The control group was matched by age and gender and consisted of 3,642 subjects (50% men, 40 ± 12 years old).
| Characteristics | Patients | Partners | Controls | CoA | TGA | MS | ES |
|---|---|---|---|---|---|---|---|
| (n = 133) | (n = 73) | (n = 3,642) | (n = 43) | (n = 42) | (n = 36) | (n = 12) | |
| Age (years) | 37 (18–75) | 37 (19–71) | 40 (19–69) | 36 (19–69) | 35 (23–75) | 39 (18–63) | 43 (23–75) |
| Men | 69 (52%) | 30 (41%) | 1,821 (50%) | 26 (60%) | 25 (60%) | 14 (39%) | 4 (33%) |
| New York Heart Association class | |||||||
| I | 102 (77%) | — | — | 39 (91%) | 31 (74%) | 32 (89%) | 0 |
| II to IV | 31 (23%) | — | — | 4 (9%) | 11 (26%) | 4 (11%0 | 12 (100%) |
| Medication | |||||||
| β blocker | 42 (3%) | — | — | 7 (16%) | 7 (17%) | 27 (75%) | 1 (8%) |
| Angiotensin-converting enzyme inhibitor/angiotensin II receptor antagonist | 54 (41%) | — | — | 13 (30%) | 21 (50%) | 16 (44%) | 4 (33%) |
| Diuretics | 8 (6%) | — | — | 3 (7%) | 3 (7%) | 0 | 2 (17%) |
| Other medication | 61 (46%) | — | — | 26 (61%) | 9 (21%) | 15 (42%) | 12 (100%) |
| No medication | 47 (35%) | — | — | 14 (33%) | 29 (69%) | 4 (11%) | 0 |
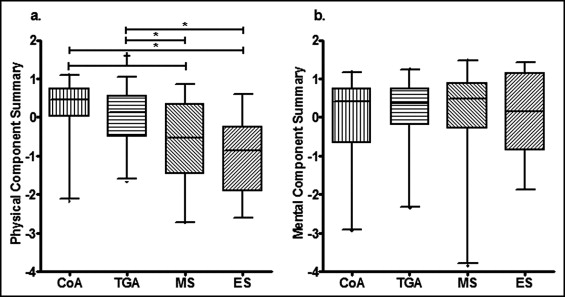
In the sexuality questionnaire, patients reported their subjective health perception to be similar compared to their partners and the Dutch population (patients 2.2 ± 0.7, partners 2.1 ± 0.7, population 1.9 ± 0.7). Patients’ SF-36 scores were significantly lower on the PCS but equal on the MCS compared to the general population (−0.2 ± 0.9 vs 0 and 0.1 ± 1.0 vs 0). Physical quality of life was particularly less in patients with Marfan syndrome and Eisenmenger syndrome, with no differences in mental quality of life among groups ( Figure 2 ).
Patients with CHD were less likely to be involved in a relationship compared to the general Dutch population (71% vs 79%, p <0.05), although those patients who were involved in a relationship perceived their relationship as more satisfactory, as did their partners (patients 4.3 ± 0.5, partners 4.3 ± 0.4, population 4.1 ± 0.6, p <0.01). Relational satisfaction was positively associated with the PCS and the MCS (r = 0.2, p <0.05, and r = 0.4, p <0.001, respectively).
The total number of sexual partners in their lifetime was significantly smaller in patients, and their partners, compared to the general population (patients 5.4 ± 7.6, partners 3.4 ± 2.9, population 7.5 ± 9.2, p <0.001). The average frequency of sexual contact in a current relationship was equal between patients and the population, with lower figures only for patients with Eisenmenger syndrome (<1 time/month, all other groups >1 time/month, p <0.05). Although sexual satisfaction was equal in patients, partners, and the population (patients 1.5 ± 0.7, partners 1.3 ± 0.5, population 1.5 ± 0.8), sexual contact caused distress in patients and their partners compared to the control group (patients 1.0 ± 1.1, partners 1.1 ± 1.1, population 0.6 ± 0.6; Figure 3 ). Sexual behavior and sexual satisfaction were important factors of quality of life, because frequency of having sexual contact was positively associated with the PCS (r = 0.2, p <0.05) and sexual satisfaction was related to the PCS, and MCS (r = 0.3, p <0.01, and r = 0.3, p <0.01, respectively). The number of sexual partners and the level of distress during sexual contact were not related to quality of life.
We found that 42% of men patients reported difficulties in obtaining and/or maintaining an erection during sexual contact, whereas 42% of partners and 54% of healthy subjects reported similar difficulties (p = NS). We found no relation among congenital cardiac defect, use of medication, or New York Heart Association (NYHA) class, and occurrence of erectile problems. There was no relation between the presence of erectile problems and quality of life. Sixty-six percent of women patients had difficulties in obtaining and/or maintaining sufficient vaginal lubrication for sexual contact versus 51% of partners and 56% of healthy subjects, which was not statistically significant. Although we found no relation between lubrication difficulties and cardiac defect or medication use, patients with lubrication difficulties had higher NYHA class (1.4 ± 0.7 vs 1.1 ± 0.2, p <0.05). Women patients with difficulties in obtaining and/or maintaining lubrication had a significantly lower MCS (−0.5 ± 1.2 vs 0.4 ± 0.8, p <0.05).
Patients with Eisenmenger syndrome had increased physical discomfort during sexual contact compared to partners and other patient groups (p = 0.01), whereas we found no differences among other patient groups. Overall, we found no relation between physical discomfort during sexual contact and age or use of medication. However, increased NYHA class was related to physical discomfort during sex (r = 0.4, p <0.001). Overall, physical discomfort during sexual contact was negatively associated with PCS and MCS (r = 0.42, p <0.001, and r = 0.3, p <0.001, respectively). Patient’s body esteem was low compared to their partners (2.5 vs 3.4, p <0.001), as was sexual esteem (3.2 vs 3.5, p <0.05; Figure 4 ). Body esteem and sexual esteem were positively associated with PCS and MCS (body esteem r = 0.3, p <0.001, and r = 0.3, p <0.001; sexual esteem r = 0.5, p <0.001, and r = 0.3, p <0.001).



