19 Septal Ablation for Obstructive Hypertrophic Cardiomyopathy
Patient Selection
1. Severe, drug-refractory cardiac symptoms (New York Heart Association functional class III/IV dyspnea or Canadian Cardiac Society angina class III/IV) due to obstructive HCM;
2. Dynamic LVOT obstruction (gradient ≥ 30 mmHg at rest or ≥ 50 mmHg with provocation) that is due to septal hypertrophy and systolic anterior motion of the mitral valve;
3. Ventricular septal thickness ≥15 mm;
4. Absence of significant intrinsic mitral valve disease;
5. Absence of the need for concomitant cardiac surgical procedure (e.g., bypass grafting, valve replacement); and
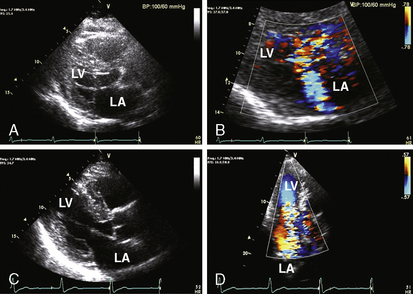
6. Informed patient consent. Informed consent requires a full understanding of the limited data on long-term survival after the procedure, the risk of pacemaker dependency, the relatively lower success rate due to its dependence on coronary anatomy, and potential complications related to cardiac catheterization and instrumentation of the coronary arteries. Although younger age has not been an absolute contraindication to the procedure, septal ablation generally has been reserved for older adult patients due to the limited data on long-term survival of the procedure. A comprehensive two-dimensional and Doppler echocardiogram is elementary to proper patient selection. This evaluation should document the dynamic nature of the LVOT obstruction and exclude anatomical findings that would impede the clinical efficacy of the procedure (Fig. 19-1).