Segmentectomy
Presentation
An 85-year-old woman with a 50-pack-per-year history of smoking has been treated with antibiotics for the past 2 weeks for symptoms of bronchitis. After a 2-week course of antibiotics, the patient’s cough persists, and a chest x-ray is obtained. The chest x-ray demonstrates a nodule in the right lung, and computed tomography (CT) scans are obtained for further evaluation.
▪ CT Scans
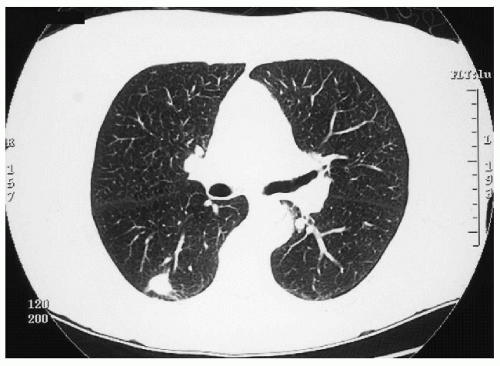 Figure 2-1 |
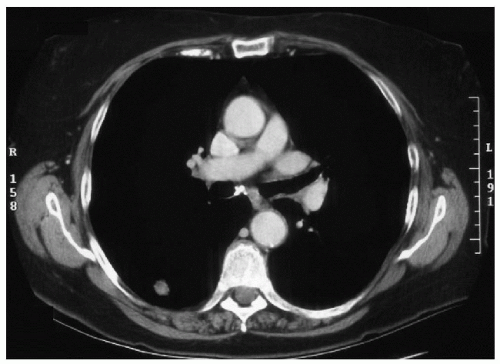 Figure 2-2 |
CT Scan Report
The CT scans demonstrate a 2-cm solitary nodule in the superior segment of the right lower lobe. The mass is spiculated and extends to the pleura. There is no mediastinal adenopathy. Mild emphysematous changes are present. There are no pleural effusions.
Case Continued
The patient undergoes a bronchoscopy, and brushing of the superior segment is negative for malignancy. Pulmonary function tests (PFTs) show a forced expiratory volume in 1 second (FEV1) of 73% of predicted and a diffusing capacity of lung for carbon monoxide (DLCO) of 60% of predicted. This is followed by video-assisted thoracoscopic biopsy and frozen section. Frozen section demonstrates squamous cell carcinoma, and the patient undergoes thoracotomy, right lower lobectomy, and medi as ti nal lymph node dissection.
At surgery, the cancer is defined as T2 N0 M0, stage IB. No radiation or chemo therapy is administered.
The patient stops smoking and returns to the clinic for surveillance chest x-ray and physical examination. Three years after surgery, the physical examination is normal, but the chest x-ray reveals an abnormality that prompts further CT scans.
▪ CT Scans
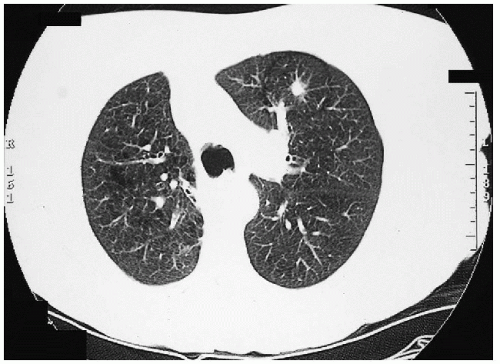 Figure 2-3 |
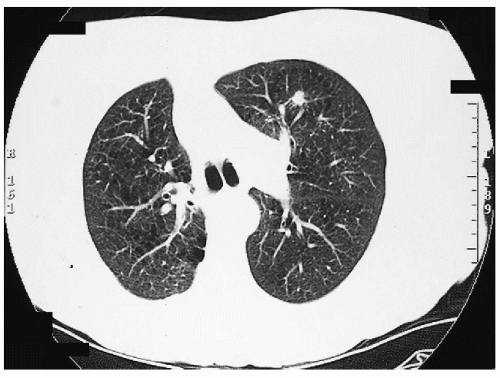 Figure 2-4
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|