Benbarkat et al reported that the Seattle Heart Failure Model (SHFM) grossly overestimated survival by 4.79 years in patients with heart failure aged >80 years. As the developer of the SHFM, I would like to correct some errors made by the investigators. The complete formula for the SHFM is available in the original report. The investigators chose to use the interactive model we developed and extrapolated for age >85 years rather than calculating the individual values. It is uncertain how much error this may have introduced in the reported values.
The SHFM reports estimated survival from 1 to 5 years and mean (average) life expectancy for a patient cohort with similar values. Mean life expectancy is the least accurate of the calculated values. Mean life expectancy is the area under the Kaplan-Meier survival curve and is quite different from median survival as reported by Benbarkat et al (the point at which 50% are alive). For example, it is possible to estimate that the mean life expectancy in this heart failure cohort is about 3.5 years, compared with the median observed survival of 1.91 years.
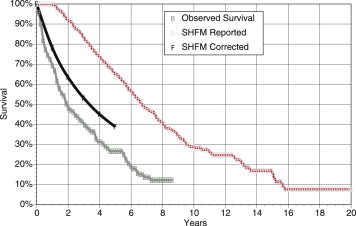
The investigators constructed a Kaplan-Meier curve using the estimated mean life expectancy rather than averaging the SHFM-estimated values for the cohort at 1 to 5 years. This error results in a Kaplan-Meier curve with SHFM-estimated 1-, 2-, and 5-year survival rates of 100%, 92%, and 65%. I have contacted the investigators, and the correct mean SHFM-estimated values for the cohort at 1, 2, and 5 years were 78.1%, 63.4%, and 38.8%, compared with the observed survival of 69.2%, 48.8%, and 26.6% (Kristian B. Filion, personal communication). As is quite evident, SHFM-predicted survival over the 1- to 5-year interval is much closer to the observed survival than depicted by the investigators ( Figure 1 ). The error at 5 years is modest, with 61% predicted mortality compared with 73% observed mortality. The SHFM median life expectancy (50% survival; Figure 1 ) is 3.45 years compared with the reported value of 6.7 years. The SHFM overestimated median survival by 1.54 years in this elderly cohort. This is much more modest than the reported 4.79 years. I would suspect that some of this error may be due to the inclusion of patients with cancer (15% of the cohort), whose deaths may be due to cancer rather than heart failure. In the Enhanced Feedback for Effective Cardiac Treatment (EFFECT) model, cancer was associated with an 85% increase in 1-year mortality. The investigators can assess this by entering the SHFM score and cancer in a Cox model or assessing the predicted and observed survival at 2 years in those with and without cancer.