Fig. 16.1
Harvested fat is separated by standard techniques before transfer
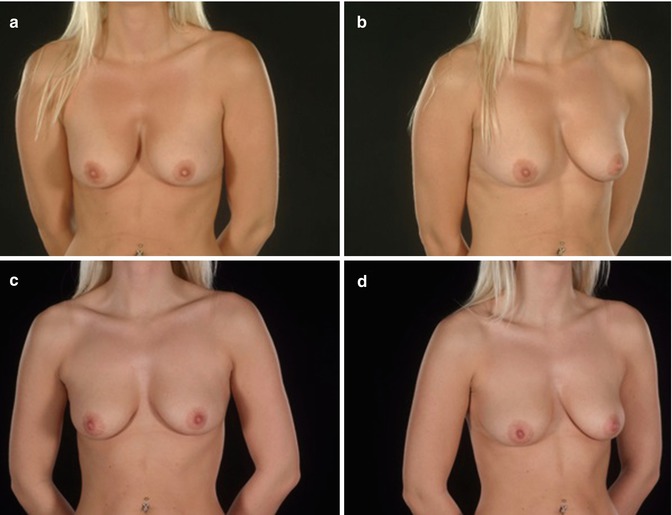
Fig. 16.2
Mild pectus excavatum in a female patient pre-operatively (a, b), and following fat grafting (c, d)
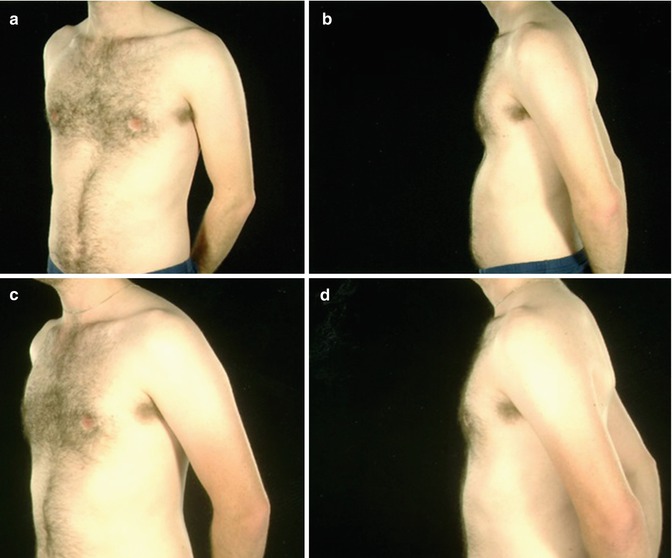
Fig. 16.3
Mild pectus excavatum in a male patient pre-operatively (a, b), and following fat grafting (c, d)
Once the transferred fat has been revascularised it may be viewed a permanent filler. However, autologous fat transfer is invariably associated with some early resorption of transferred fat, and a degree of “over augmentation” is advised. Despite this, it is likely that repeated procedures will be required. The complications of fat grafting, including fat necrosis, cyst formation and calcification are well recognized and rarely cause significant morbidity. Transferred fat cells will be subject to hypertrophy and atrophy as body weight changes. The major advantage of fat grating is than it removes any longer term implant related problems. The presence of adipose derived mesenchymal stem cells (ADMSC) within the transferred fat, play an adipogenic and angiogenic role, are thought to be largely responsible for graft survival and stem cell enriched fat grafts have become increasingly used. Transferred fat has had reportedly positive restorative effects on surrounding soft tissues, particularly in previously irradiated areas or heavily scarred chronic wounds.
Flap Transfer
Given the relative successes of the aforementioned techniques flap reconstruction is less commonly used in these cases. An occasional exception is Poland’s syndrome. Bipolar transfer of the latissimus dorsi muscle (LD) can reconstruct the anterior axillary fold and provide some bulk to replace the absent pectoralis major in these patients. The LD is raised as a muscle flap and rotated on its thoracodorsal pedicle to the front of the chest. The key step to provide a satisfactory contour of the anterior axillary fold involves detaching the LD from its humeral insertion and reattaching on the bicipital groove anterior to the neurovascular bundle. Although this transfer has been described as a functional reconstruction for the absent (or hypoplastic) pectoralis major, it is primarily used for aesthetic purposes. The LD muscle can also be affected in Poland’s syndrome and its presence and bulk should be confirmed clinically prior to planning any surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


