Chapter 25 Rigid Bronchoscopy for Removal of a Foreign Body Lodged in the Right Lower Lobe Bronchus

Case Description
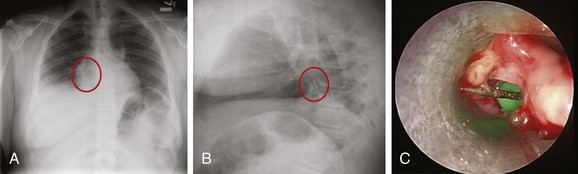
A 14-year-old male with a past medical history of asthma developed acute cough and wheezing immediately following an episode of intense laughter. Actually, he was holding a thumbtack between his teeth when his brother made a funny comment. Bursting into laughter, he suddenly aspirated the thumbtack. He did not tell his parents. Several days later, his intractable cough prompted his parents to bring him to the hospital, where he told physicians about the accident. Flexible bronchoscopy revealed the foreign object in the distal left main bronchus, but despite multiple attempts, it could not be removed and was inadvertently dropped over and into the right bronchial tree. He was transferred to our facility a few days later. His vital signs showed a BP of 150/85, HR of 110, RR of 22, temperature of 100.5° F, and O2 sat of 94% on room air. On examination, he had no wheezing, but air entry at the right base was diminished. The child was a nonsmoker and had no significant family history. His asthma was well controlled on inhaled fluticasone 110 mcg twice a day, with which he was usually noncompliant. Laboratory data were normal, except for a WBC of 18,000. Chest radiograph showed a radiopaque object projecting over the right lower lung field (Figure 25-1). During rigid bronchoscopy, a thumbtack surrounded by inflamed mucosa and granulation tissue was found and was causing complete obstruction of the right lower lobe bronchus (see Figure 25-1).
Discussion Points
1. List five accessory instruments that can be used to remove a foreign body from the airway.
2. List three complications that might occur during attempts to remove a sharp or pointed object from a lower lobe bronchus.
3. Describe the advantages and disadvantages of flexible bronchoscopy and rigid bronchoscopy for removing aspirated foreign bodies.
Case Resolution
Initial Evaluations
Physical Examination, Complementary Tests, and Functional Status Assessment
This patient’s presentation was classic for foreign body aspiration (FBA), defined as the inhalation of an organic or inorganic foreign object into the larynx and respiratory tract.1 The object was in the right lower lobe, but when a foreign body is in the trachea, patients may have a brassy cough, with or without loss of voice, and bidirectional (during inspiration and expiration) stridor. Complete airway obstruction and asphyxia can develop when a large object is lodged in the trachea or larynx.2 Cyanosis, stridor, and altered level of consciousness are ominous signs and predict impending respiratory arrest.
As in this case, signs predictive of bronchial FBA include radiopaque objects seen on chest x-ray (CXR), a history of FBA associated with unilaterally decreased breath sounds, localized wheezing, focal hyperinflation, and atelectasis (this is usually a later finding, which occurs after air has been resorbed). Prompt diagnosis is essential, especially in children, because results from studies show that complication rates are twofold higher in patients who receive medical attention 2 or more days after the aspiration, compared with patients cared for sooner.3 Physical examination in patients with bronchial FBA may reveal unilateral wheezing, which suggests partial airway obstruction distal to the carina.4,5 By the time our patient came to our institution, wheezing had ceased, probably complete obstruction had developed, and there was no longer any airflow to the right lower lobe (RLL) bronchus.
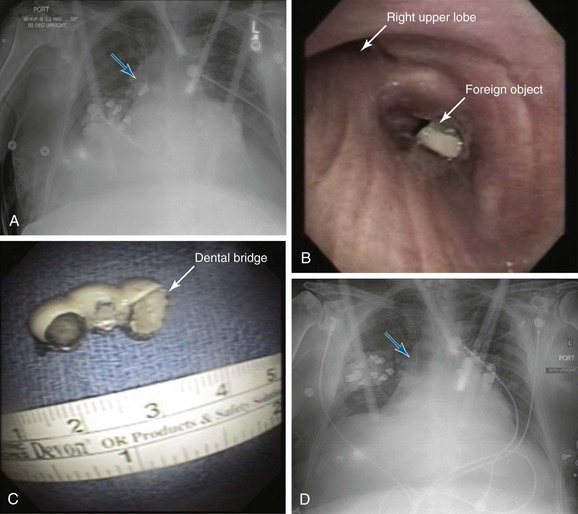
Chest radiograph is a commonly performed imaging modality for suspected FBA in a stable patient. Standard frontal and lateral views can help locate the object (see Figure 25-1).4 Lateral soft tissue views of the neck are performed if upper airway involvement is suspected clinically. If the patient is critical and suspicion for FBA is high based on the history and physical examination, CXR is not absolutely necessary, and airway management should take priority. Characteristic findings on CXR depend on the density of the aspirated object and on the duration of symptoms. Radiopaque materials such as coins, thumbtacks, metallic nails, toys, bones, teeth, and dental appliances usually can be detected on radiographs. Radiopaque foreign bodies, however, are seen in only 2% to 19% of patients with FBA because most aspirated objects are radiolucent. Furthermore, radiopaque material seen on x-ray may actually represent calcifications of mucoid impaction or a broncholith, and thus could be a false-positive finding. In fact, the sensitivity of CXR performed in the emergency department for FBA is reportedly only 22.6%. False-negative rates vary between 5% and 30% in children and between 8% and 80% in adults, probably because of differences in physical properties of aspirated materials. For example, organic materials such as meat and vegetables are difficult to visualize because they are not radiopaque.6,7 When the aspirated material is radiolucent and is not identified on chest x-ray, nonspecific CXR findings that suggest FBA include atelectasis, pneumonia, air trapping, and pneumomediastinum. Air trapping is an early radiographic finding that results from obstruction of the airway by the foreign body, which acts as a ball valve, allowing air to enter the bronchus but not to exit during expiration. Expiratory and inspiratory chest x-rays, when feasible, may help detect any air trapping.8 In children with aspirated foreign bodies, the absence of air trapping was found to have a negative predictive value of 70%.9 However, because overall sensitivity is low, a normal CXR, does not preclude additional diagnostic studies such as chest computed tomography (CT), which can detect foreign bodies not visualized on CXR in up to 80% of cases.10 This modality is particularly useful in patients with chronic respiratory symptoms or with recurrent pneumonia. False-negative CT scans, especially with 10 mm slice thickness, may occur because CT can miss small objects, and because image quality is compromised by motion artifacts in patients with severe dyspnea.4 CT findings include visualizing the foreign body in the airway lumen and observing indirect findings such as atelectasis, hyperlucency, bronchiectasis, lobar consolidation, tree-in-bud opacities, ipsilateral pleural effusion, ipsilateral lymphadenopathy, and thickening of the bronchial wall adjacent to the foreign body.
In children, low-dose multidetector CT (MDCT) scanning and virtual bronchoscopy (VB) (Figure 25-2) have a sensitivity of 92% to 100% and a specificity of 80% to 85%.11,12 False-positives occur because of secretions and endobronchial tumors. Therefore MDCT and VB, if available and when feasible, can be used as noninvasive tools to confirm FBA and to determine the exact location of the obstruction before bronchoscopy. Some authors suggest that in the presence of a positive clinical diagnosis and a negative CXR, VB should be considered in all children with suspected FBA to avoid a potentially unwarranted rigid bronchoscopy.12
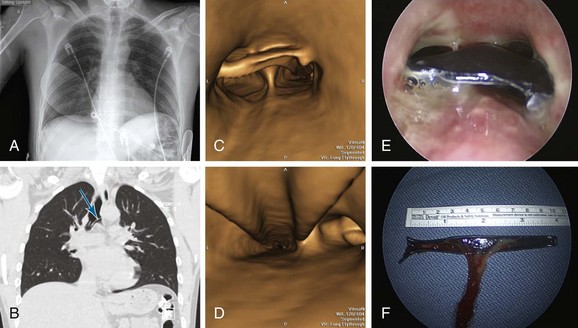
In stable adults, flexible bronchoscopy should be used to confirm suspected cases of FBA and to attempt removal of the foreign body.4 This is also true for victims of cervicofacial trauma (Figure 25-3). Rigid bronchoscopy usually is not indicated in these patients because of neck immobilization. In addition to allowing removal of the FB, bronchoscopy determines the exact nature of the foreign body, its location and degree of airway obstruction, and associated mucosal abnormalities such as surrounding mucosal edema and granulation tissue (see Figure 25-3). In patients presenting with acute asphyxia, flexible bronchoscopy or rigid bronchoscopy can be performed, depending on availability. In stable children with suspected FBA, flexible bronchoscopy has been shown to safely confirm the diagnosis and has been used to extract foreign objects5; it provides rapid and definitive diagnosis of FBA in approximately 12% of children who present with persistent wheezing (lasting longer than 6 weeks and not responding to bronchodilators and inhaled corticosteroids).13 Controversy continues, however, because some authorities recommend rigid bronchoscopy in children younger than 12 years of age when there is a strong suspicion of FBA, arguing that rigid bronchoscopy permits better control and visualization of the pediatric airway.14
Comorbidities
Our patient had controlled asthma on inhaled corticosteroids. Although acute asthma exacerbation was in the differential diagnosis, wheezing in asthma is usually paroxysmal, intermittent, and diffuse and improves after bronchodilators. Symptoms are triggered by exercise, cold, sleep, and allergens, and the CXR usually shows peribronchial cuffing and bilateral hyperinflation. The presence of these findings, however, would not rule out FBA.15 Indeed, dyspnea alters the coordination between deglutition and respiration, increasing the risk for aspiration.16
Our patient had no evidence of dysphagia or impaired cough reflex.4 These conditions are usually seen in the elderly, especially in cases of cerebrovascular or degenerative neurologic disease. More than one third of patients with acute stroke have radiologic evidence of aspiration.17 Patients with dysphagia have delayed triggering of the pharyngeal motor response and decreased laryngeal elevation, resulting in poor coordination and timing of oral, pharyngeal, and laryngeal movement during swallowing.18 Anticholinergics, antipsychotics, and anxiolytics also impair the cough reflex and/or swallowing.
Procedural Strategies
Indications
Although some controversy continues, most clinicians agree that rigid bronchoscopy is indicated in patients with FBA associated with stridor or asphyxia, as well as in children with radiopaque objects seen on CXR (because the diagnosis is obvious), a history of FBA associated with localized wheezing, obstructive hyperinflation, atelectasis, or unilaterally decreased breath sounds suggesting mainstem bronchial obstruction. Large, round, or smooth foreign bodies probably are best approached with the rigid bronchoscope (see video on ExpertConsult.com) (Video VI.25.1 ).
).
In other cases, flexible bronchoscopy should be performed to confirm the diagnosis and attempt removal. Although this procedure is safe, effective, and cost-effective, dislodgment and unsuccessful retrieval of the object are possible.14 Potential complications of attempting to remove large foreign bodies with a fiberoptic bronchoscope include displacement or impaction of the foreign body in a lobar or mainstem bronchus, shearing off of the foreign body in the narrow subglottic area, and acute asphyxia from subglottic or laryngeal obstruction.19 If flexible bronchoscopy fails, rigid bronchoscopy is warranted.9 Advantages of rigid bronchoscopy include the ability to function as an endotracheal tube, securing the airway and providing a conduit through which the foreign body can be removed using a variety of larger instruments. As mentioned earlier, however, flexible bronchoscopy remains the method of choice for patients with cervicofacial trauma (see Figure 25-1) and for those who are already intubated.4
Contraindications
This patient’ s asthma was not a contraindication to bronchoscopy, but optimal control before the intervention is warranted; studies have shown that even patients with mild asthma have a more pronounced post bronchoscopy decrease in forced expiratory volume in 1 second (FEV1) compared with normal subjects. Reductions in FEV1 and forced vital capacity (FVC) are especially greater after bronchioloalveolar lavage and biopsies.20 Bronchoscopy is safe in asymptomatic asthmatic patients with FEV1 >60% predicted.21 Premedication with bronchodilators was associated with no fall in post procedure FEV1.22 This is different from COPD, in which premedication with an inhaled short-acting agonist is not routinely recommended (in COPD, bronchodilators have not been shown to affect post procedure reduction in FEV1).23
If patients have active diffuse wheezing, premedication with nebulized bronchodilators is warranted, and in elective cases, the procedure might have to be postponed until bronchospasm is controlled. One large study found that bronchoscopic interventions in asthmatic patients were associated with significantly higher rates of procedure- or anesthesia-related complications such as laryngospasm or bronchospasm, status asthmaticus, severe hypoxemia, and cardiac arrest, compared with interventions in nonasthmatic patients.24
Expected Results
Both flexible and rigid bronchoscopy can be performed for removal of foreign bodies, but overall, flexible bronchoscopy seems to be an efficient initial method in both children and adults, with a success rate greater than 90%.5,25 Repeated bronchoscopic examination may be necessary to remove a foreign body completely in 1% to 3% of patients, especially if the foreign body is a peanut or another material that breaks easily.9,14 When flexible bronchoscopy fails, rigid bronchoscopy should be performed,9 as was done in this case. Open surgical interventions are very rarely necessary and are reserved for repeatedly unsuccessful bronchoscopic interventions.
Complications of FBA are usually prevented by prompt removal of the object. A retained object can lead to prolonged atelectasis and lung destruction, occasionally requiring thoracotomy and resection. Early complications of FBA include asphyxia, cardiac arrest, laryngeal edema, and pneumomediastinum. Organic objects, especially those with high oil content such as peanuts, may cause significant mucosal inflammation and bulky granulation tissue growth within a few hours, eventually causing complete bronchial obstruction. Late complications include bronchiectasis, hemoptysis, bronchial stricture, and inflammatory polyps. Objects can change sides, moving from left to right or from right to left, or can migrate distally, causing complete obstruction and atelectasis.14 Table 25-1 summarizes potential complications associated with FBA.
Table 25-1 Potential Complications Due to Foreign Body Aspiration and Its Bronchoscopic Removal
| Complication | Comments |
|---|---|
| Asphyxia | Aspiration of a foreign body is the fifth most common cause of mortality from unintentional injury in the United States, and it is the leading cause of mortality from unintentional injury in children younger than 1 year. |
| Pneumonia | Seen in 20% of patients who present days or weeks after FBA.7 The incidence may be higher with delayed presentation. |
| Atelectasis | Complete obstruction from the foreign body or associated secretions and granulation tissue can cause atelectasis, seen in approximately 20% of patients on CXR and in approximately 60% on chest CT scan.4 |
| Bronchiectasis | On chest CT, this is a late complication that can be seen in about 30% of patients with FBA; occasionally, severe and recurrent infections may require thoracotomy and pulmonary resection. |
| Pneumomediastinum | A rare acute finding on CXR in approximately 3% of patients with FBA.7 |
| Subglottic edema related to rigid bronchoscopy | Between 2% and 4% of patients requiring rigid bronchoscopy for foreign body extraction develop laryngeal edema that requires brief intubation and admission to intensive care.9 |
| Bronchoscopy-related bronchospasm | More than 4% of children who require rigid bronchoscopy for foreign body extraction develop bronchospasm.9 |
| Bronchial stricture | Aspiration of iron or potassium-chloride pills can cause airway inflammation, resulting in fibrosis and bronchial strictures. |
CT, Computed tomography; CXR, chest x-ray; FBA, foreign body aspiration.
Team Experience
Access to both flexible and rigid bronchoscopy is warranted, especially if the bronchoscopist is inexperienced or unskilled in flexible foreign body retrieval. Consultation with a rigid bronchoscopist, who may be a pulmonologist, a thoracic surgeon, or an otorhinolaryngologist, can help in developing a management strategy. Care should always be taken to avoid inadvertently pushing foreign objects more distally into the airway because this will make subsequent retrieval more difficult. Communication among team members is essential. For example, several different foreign body removal accessory instruments should be available, and one should not assume that simple grasping forceps will suffice. If procedures are being performed with the patient under general anesthesia, it may be necessary to cease ventilation to avoid blowing the object away from the grasping instrument. Wedging the foreign object into the rigid bronchoscope or endotracheal tube before removal may be necessary to avoid laryngeal or airway wall injury; sometimes, it is preferable to remove the tube and foreign body en bloc, rather than attempt to remove the foreign body alone. At other times, if the bronchoscopist is taking too long to grasp the object in a distal airway and ventilation is inadequate, a momentary retreat to the mid-trachea is warranted, so the anesthesiologist can ventilate the lungs adequately.26 If a forceps and a bronchoscope are removed en bloc, along with the foreign body, the bronchoscopist should ask the anesthesiologist to deepen the level of anesthesia to avoid bucking or coughing, which may result in dropping of the foreign body back into the airway or inadvertent traumatizing of a closing glottis. Care must also be taken to avoid losing the foreign body in the oral pharynx once the vocal cords have been passed. The foreign object should always be kept in view and grasped firmly. One should be ready to remove the object from the oral cavity using one’s fingers, a Magill forceps, a rigid laryngoscope, or the rigid bronchoscope. It may be necessary to pull the tongue outward (using a gauze to hold the tip of the tongue firmly between one’s index finger and thumb) to create more space in the oropharynx. A retrieval strategy should be shared with the team. For example, we have seen (1) foreign bodies removed by flexible bronchoscopy performed through the nares; once the foreign body is grasped, it is discovered that it is too large to be removed through the nares and thus must be dropped into the oral cavity and extracted, spit out, or accidentally swallowed; (2) foreign bodies grasped with forceps, only to be wedged within the subglottis, causing acute asphyxia; (3) sharp objects stabbing the inferior aspect of the glottis because the object is removed tangentially to the airway in an unprotected fashion; and (4) flexible bronchoscopes being broken because the foreign body is released into the oropharynx. During retrieval, the bite block was loosened and retracted proximally, which exposed the scope to a patient’s teeth during a violent cough.
Therapeutic Alternatives for Foreign Body Removal
1. Flexible bronchoscopy is the method of choice in a patient with cervicofacial trauma because rigid bronchoscopy would be impossible in such a patient, and the only alternative is open thoracotomy. Flexible bronchoscopy is also a reasonable first therapeutic choice in a patient with a foreign body lodged in the distal airways.4 Because patient cooperation facilitates foreign body retrieval by flexible bronchoscopy, this method may not be ideal in very young children.
2. Surgery is indicated if repeated flexible and rigid bronchoscopic attempts fail. Thoracotomy with pulmonary resection is usually reserved for cases of a destroyed pulmonary segment or lobe, or damage to the entire lung.27
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


