(1)
Department of General surgery, Fuwai Hospital, Beijing, China
17.1 General Considerations
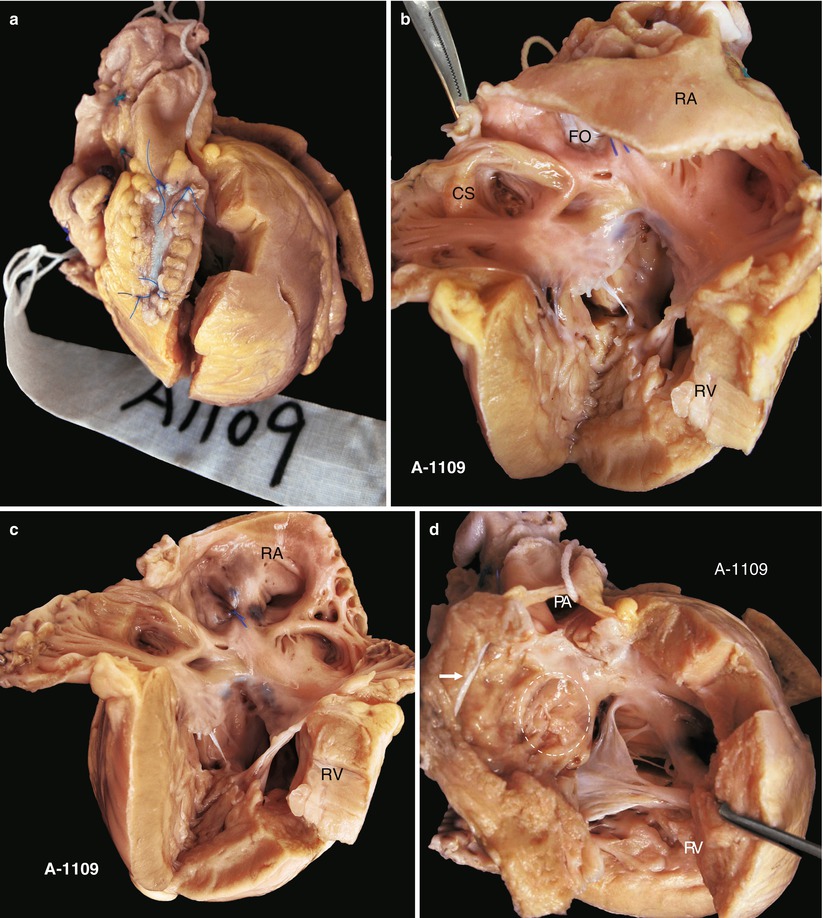
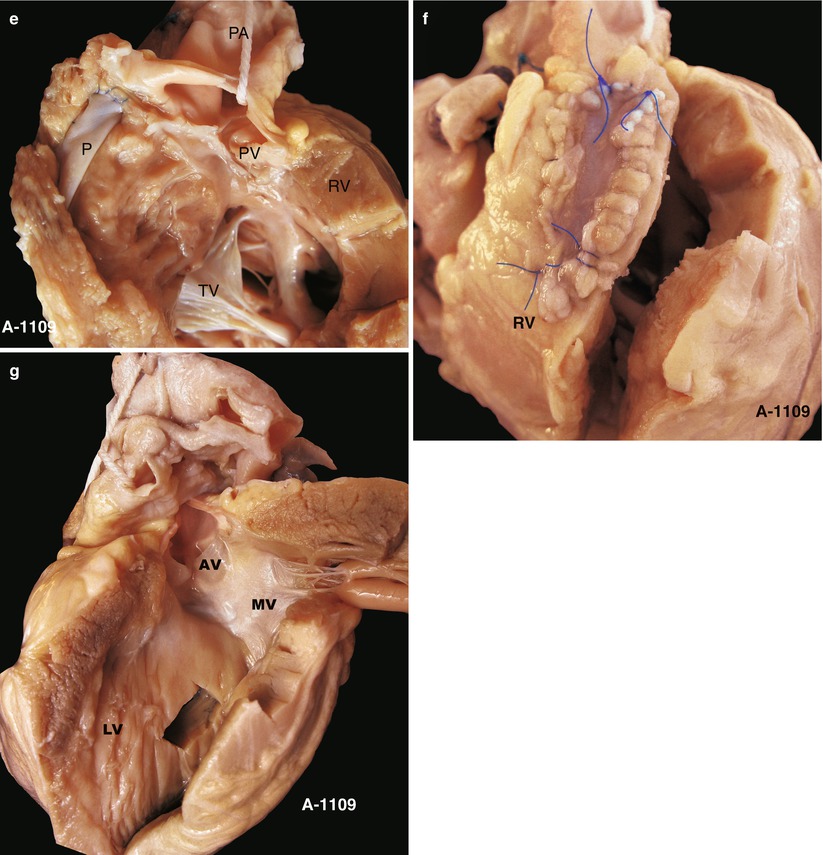
In this chapter, we will discuss congenital RV infundibulum muscular hypertrophy stenosis, including the muscle bundle of the muscular ventricular septum, combined with the main pulmonary stenosis, ASD or VSD. There is no RV or TV aplasia or dextropositioned aorta such as TOF, pulmonary atresia, or transposition of the great arteries (TGA) (Fig. 17.1a–g).
17.2 Embryology
Right ventricular outflow also means the right ventricular infundibulum, which originates from the circular cone of the primitive heart tube. The circular cone resides on the left and right ventricles, and the conical septum divides the circular cone into the pulmonary circular cone (right ventricular infundibulum) and the aortic circular cone (left ventricular outflow). If the course does not proceed successfully, the pulmonary circular cone will be smaller. The last growth stage of the circular cone is a rotation forward of the pulmonary circular cone and the absorption of the aortic circular cone. If muscular hypertrophy occurs under the pulmonary circular cone, right ventricular infundibulum stenosis or obstruction will occur (Fig. 17.2). This chapter discusses mainly abnormal infundibulum pachynsis, not rotation or lack of absorption (Fig. 17.1d).
The right ventricular infundibulum is a circular muscular structure composed of muscular fiber and located between the pulmonary and the tricuspid valves. Its outer layer is circuitous muscle, and the inner layer is composed of circuitous and oblique muscle. The septal band passes through the ventricular septum, the parietal band forms the anterior wall of the RVOT, and the oblique band is included in the diagonal muscle. The oblique band originates from the ventricular septum and passes across the entire RV and adheres to the root of the anterior leaflet of the TV, which is called the moderator band. The congenital proliferation of the muscle band leads to outflow tract obstruction. The abnormal right ventricular band is defined as an abnormal moderator band that obstructs between inflow and outflow, which separates the RV into two cavities. It is very important to distinguish the abnormal band because we regard the narrow outflow tract as a VSD at times (Fig. 17.3).
17.3 Types of Infundibulum Obstructions
17.3.1 Entrance Obstruction (Fig. 17.4)
The entrance is a fibrous muscular ring that lies on the papillary muscle of the conus arteriosus. The infundibulum is normal, and the hollow can be seen on the surface of the wall; the hole is limited, followed by secondary pachynsis of the proximal muscle, but a normal or larger cavity is seen in the far end.
17.3.2 Tube-Like Obstruction (Fig. 17.5)
A tube-like obstruction involves mainly the muscular pachynsis all around, but with no expansion after the main pulmonary artery in most cases.
17.3.3 Limited Stenosis Under the Pulmonary Valve (Fig. 17.6)
This obstruction involves a fibrous muscular ring or occasionally only a fibrous membrane. The obstruction could be exposed through an incision of the pulmonary artery. The hemodynamics of obstruction under the PV and simple pulmonary obstruction are nearly the same, so there is expansion after the main pulmonary artery.
17.4 Specimen Demonstrations
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


