Right Middle Lobe Syndrome
Jonathan H. Chung, MD
DIFFERENTIAL DIAGNOSIS
Common
Middle Lobe Syndrome
Central Obstruction
Extrinsic Obstruction by Lymph Nodes
Bronchostenosis
Endobronchial Mass (Tumor or Foreign Body)
Peripheral Obstruction
Pneumonia (Mimic)
Atelectasis (Mimic)
Less Common
Pectus Excavatum (Mimic)
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Recurrent or chronic atelectasis of right middle lobe &/or lingula
Due to extrinsic compression, central obstruction, or peripheral obstruction
Peripheral obstruction from lack of collateral ventilation due to complete fissures hampering clearance of secretions during coughing
60% benign etiology (e.g., tuberculous stricture, nodal compression)
Helpful Clues for Common Diagnoses
Middle Lobe Syndrome
Chronic or recurrent volume loss in right middle lobe or lingula; often associated with bronchiectasis
Triangular opacity, which silhouettes right heart border on frontal chest radiograph
Wedge-shaped opacity overlying heart on lateral chest radiograph
CT may demonstrate endobronchial mass, lymph node, or broncholithiasis obstructing proximal bronchus
Pneumonia (Mimic)
Ground-glass opacities to dense consolidation within right middle lobe or lingula
Reactive lymphadenopathy; very large lymph nodes unusual
Parapneumonic pleural effusion or empyema
Atelectasis (Mimic)
Volume loss in right middle lobe or lingula
In acute setting, most often due to central mucous plugging or aspirated material
Similar imaging findings as in middle lobe syndrome
Mild reversible dilation of airways; not as severe as bronchiectasis in middle lobe syndrome
Helpful Clues for Less Common Diagnoses
Pectus Excavatum (Mimic)
Sternum depressed posterior to anterior ribs
Right heart border obliterated as sternum displaces lung from right heart border
Cardiac displacement and rotation may give false appearance of cardiomegaly
Image Gallery
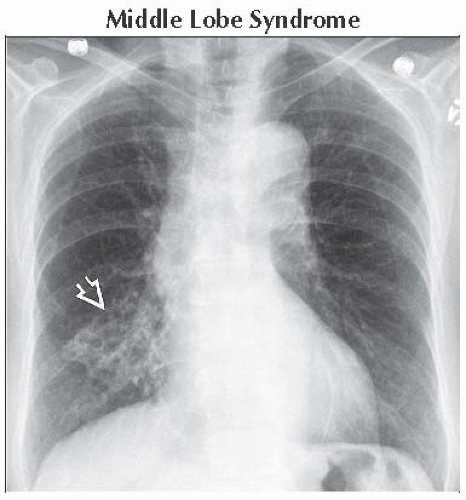 Frontal radiograph shows a triangular opacity
 partially silhouetting the right heart border. There are internal cystic and tubular lucencies suggestive of bronchiectasis. partially silhouetting the right heart border. There are internal cystic and tubular lucencies suggestive of bronchiectasis.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|