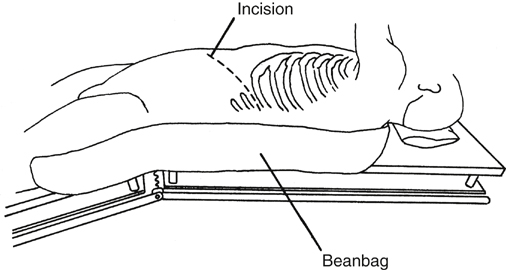
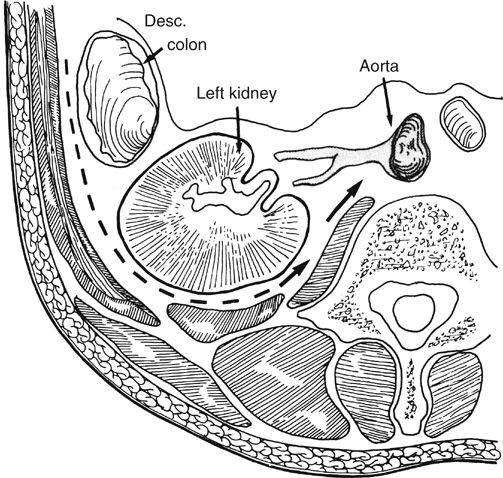
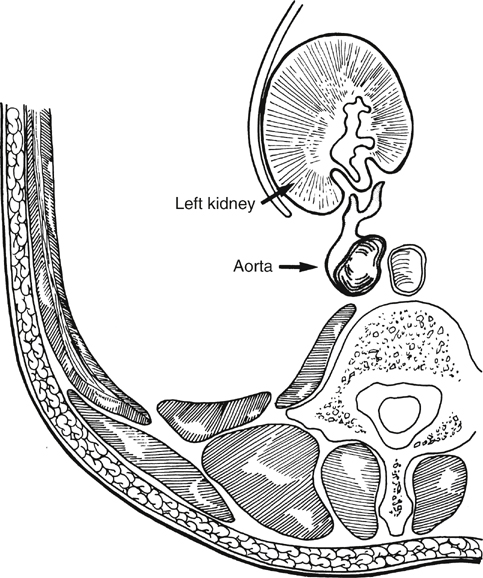
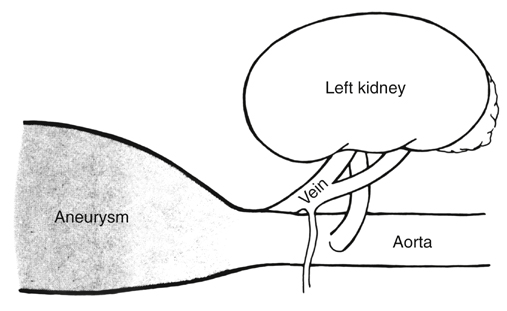
After the induction of general anesthesia, the patient is placed on a suction bean bag (Olympic Vac Pac, Marlin Medical, Victoria, Australia) in a modified right lateral decubitus position. The patient is positioned with the table break 5 to 10 cm cephalad to the left iliac crest (Figure 1). The patient’s torso is elevated 45 to 60 degrees from the horizontal position, and the pelvis is rotated 15 to 30 degrees to allow access to both groins. The left upper extremity is brought across the chest and supported by blankets or a stand. The left thigh is elevated above the horizontal plane by means of blankets or an additional suction beanbag to relax the ipsilateral iliopsoas muscle and improve access to the distal aorta and left iliac arteries. To open the space between the iliac crest and the costal margin, the table is flexed 20 to 30 degrees in a reverse V position at the table break. The retroperitoneal space is entered posterolaterally to avoid tearing the parietal peritoneum (Figure 2). The posterior peritoneum, posterior layers of Gerota’s fascia, and the left kidney are retracted anteriomedially and cephalad to expose the left psoas muscle and periaortic tissue. The fascia remains intact on the psoas, which minimizes dissection-related injury of the genitofemoral nerve and bleeding from the iliopsoas muscle. Exposure is maintained with a self-retaining retractor. Care must be taken to avoid vigorous retraction of the anterior and cephalad margin of the incision because this can result in injury to the spleen or kidney. After systemic anticoagulation with heparin, the outflow is occluded and the neck of the aneurysm is approached posterolaterally (Figure 3). The landmarks for the infrarenal neck of the aortic aneurysm are the origin of the left crus of the diaphragm, the lumbar branch of the left renal vein, and the left renal artery (Figure 4). The lumbar branch of the left renal vein, which crosses the aorta in a posterior and perpendicular fashion and caudad to the renal artery, is ligated and divided. The lymphareolar tissue is dissected to expose the proximal infrarenal aorta. The left lateral side of the aorta is dissected, followed by anterior and then posterior dissection of the aorta from the surrounding tissues.
Retroperitoneal Approach for Elective Abdominal Aortic Aneurysmectomy
Surgical Techniques
Left Posterolateral Retroperitoneal Approach
Exposure
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Retroperitoneal Approach for Elective Abdominal Aortic Aneurysmectomy