■ For thoracoabdominal exposure, the patient is placed in the right lateral decubitus position using a beanbag and axillary role for support. The left arm is protected with adequate padding and an airplane-type retractor. It is important to secure the left arm such that the scapula rolls anteriorly, providing exposure of the posterior lateral chest. The incision will be made overlying the 8th intercostal space and extended toward the umbilicus.
TECHNIQUES
■ The incision is carried through the external oblique, internal oblique, and transversus abdominis muscles. The retroperitoneal space is then entered laterally near the tip of the 11th rib by identifying the characteristic yellow preperitoneal fat. The retroperitoneal space is then developed from lateral to medial using a sponge stick or hands for blunt dissection. Anteriorly, the peritoneum tends to be more adherent at the level of the rectus sheath; care should be taken to avoid entering the peritoneal cavity in this area. The psoas fascia is encountered as the dissection is developed posteriorly in the course of this dissection, which leads directly to the left iliac vessels and ureter. Dissection is continued proximally anterior to the ureter; the ureter is either left in situ to limit injury or gently retracted medially with silastic slings as the retroperitoneal space is developed.
■ Superiorly, the kidney is identified as the dissection is continued anterior to Gerota’s fascia—a potential space exists between descending colon and Gerota’s fascia in the retroperitoneum, which is progressively developed in a cephalad direction from the psoas muscle, adjacent to the aorta. Once the renal vein is visualized in this space, the superior margin of the dissection is complete. If suprarenal aortic control and exposure is required, this same dissection plane should be developed posterior to the kidney, elevating the kidney and ureters along with the peritoneal contents and retracting all to the right to expose the subdiaphragmatic visceral aorta.
■ Self-retaining retractor systems are best deployed either after the psoas muscle is identified or following exposure of the renal vein or elevation of the left kidney. Deploying the retractor system earlier will interfere with the dissection necessary to access the appropriate retrocolic space. Following placement of the initial padded retractor blade along the medial margin of the wound, circumferential retraction is secured by placement of additional blades, typically opposite each other to prevent undue tension on the retraction system, with sequential replacement with deeper blades and additional retraction until the entire periaortic retroperitoneum is exposed.
■ The aorta and iliac arteries are then dissected free of surrounding tissue. Circumferential aortic control is an essential safety element of all aortic procedures, and care should be taken to gently and patiently create a space between the inferior vena cava (IVC), aorta, and vertebral bodies posteriorly to pass an umbilical tape around the aorta with a right-angle clamp. Circumferential control of the common iliac arteries, on the other hand, is not necessary in all circumstances. Sufficient medial and lateral dissection to allow for placement of a Wylie hypogastric clamp around the common iliac artery will usually suffice. Avoidance of attempts at circumferential iliac control will reduce the risk of right iliac vein injury. When circumferential control is required, patience is necessary to gradually separate the right common iliac artery from the distal IVC and left common iliac vein. When a venous injury is encountered during this maneuver, division of the common iliac artery may be necessary to gain adequate exposure for control. Alternatively, an occlusion balloon may be introduced from the right common femoral or external iliac veins will tamponade the venous bleeding until sufficient exposure is gained to repair the wound. Finally, a covered self-expanding endograft may also be deployed over a wire to gain control. Again, readjustment of the retractor system with each consecutive stage of exposure will optimize operative efficiency. Frequently, to optimize distal exposure, the proximal retractor blades need to be temporarily relaxed and vice versa.
■ This exposure provides adequate exposure to the infrarenal aorta (and inferior mesenteric artery if reimplantation is anticipated), right and left common and left external iliac arteries. The right external iliac artery is not well visualized from this approach, although tunneling to the right femoral artery is readily achieved for aortofemoral bypass grafting when necessary. Care should be taken to develop the tunnel immediately anterior to the iliac arteries to avoid injury to the right ureter or trapping the ureter between the graft limb and adjacent artery. When right external iliac artery exposure is required during a left retroperitoneal exposure, a counterincision may also be placed in the right lower quadrant, although patient positioning and retractor system placement may limit the potential use of this maneuver.
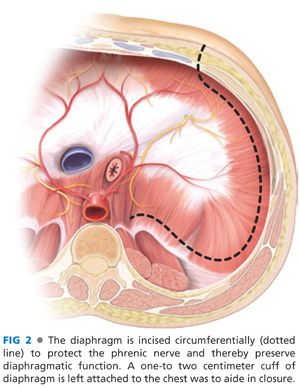
■ For procedures requiring more proximal, visceral aortic exposure, the latissimus dorsi is identified and dissected from surrounding superficial and deep tissues and retracted laterally. The 8th intercostal space is opened posteriorly to the paraspinal muscles and anteriorly to the costal margin, which is divided. As the retroperitoneal space is developed, the peritoneum is bluntly separated from the inferior surface of the diaphragm. The diaphragm is divided in a circumferential manner 1 to 2 cm from its attachments to the chest wall to avoid injury to the phrenic nerve (FIG 2). The median arcuate ligament is identified and divided. Proximal aortic control can now be obtained under direct vision, again following strategic placement of self-retaining retractor blades, taking care to identify and avoid injury to the esophagus.
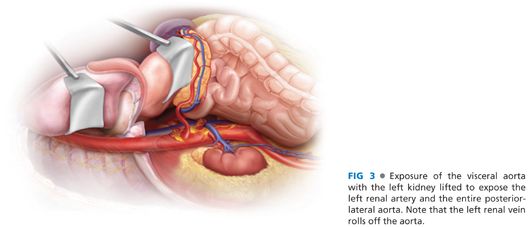
■ Dissection of the plane posterior the Gerota’s fascia allows for exposure of the left renal artery, which is an important landmark in further dissection of the visceral aorta. Once the origin of the left renal artery is identified and the median arcuate ligament has been divided, the visceral aorta and origins of the celiac axis and SMA can be isolated with sharp dissection. With the left kidney rotated anteriorly, the SMA can be exposed over a distance of approximately 5 cm (FIG 3). Additional exposure can be obtained by rotating the kidney posterior to expose the SMA as it courses behind the pancreas (FIG 4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


