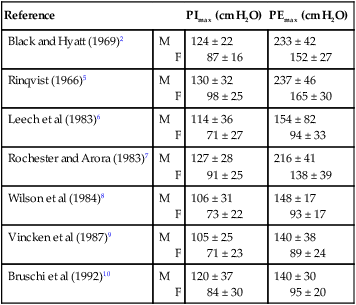
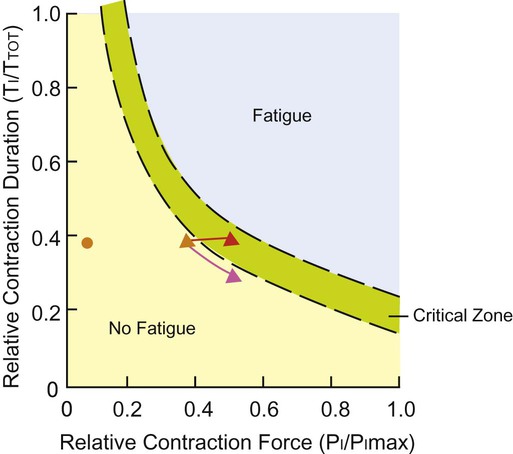
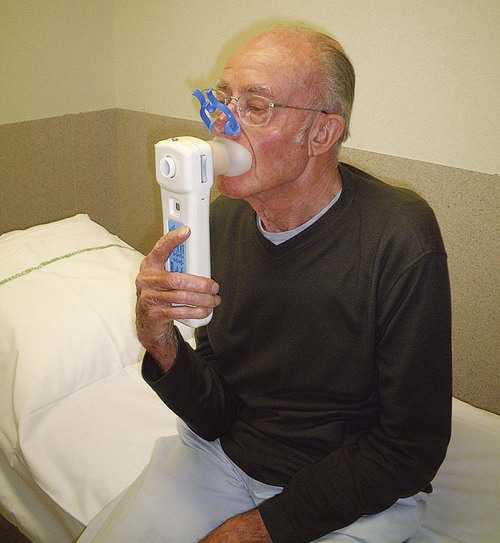
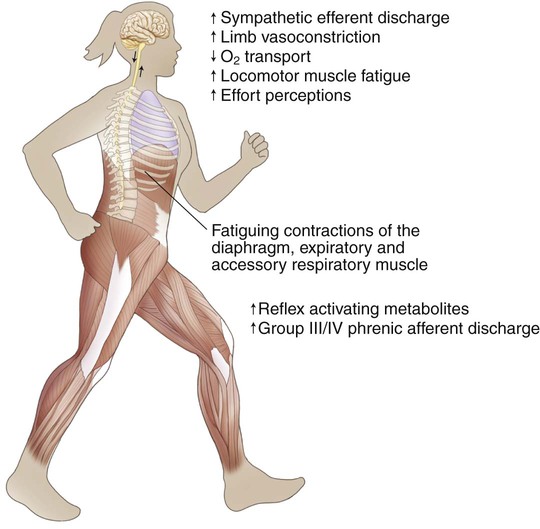
The capacity of the respiratory muscle pump is vital for the movement of air to the level of gas exchange in the respiratory system. Impairment of the respiratory pump compromises ventilation, gas exchange, and tissue respiration. The respiratory muscles drive ventilation. In conditions where the load on the respiratory muscles is increased or the capacity of the respiratory muscles is decreased, muscle weakness can occur. Breathing pattern (i.e., rapid shallow breathing) adapts, however, to help counter respiratory muscle fatigue.1 Although this adaptation decreases the effectiveness of gas exchange, a breathing pattern with a lower tidal volume and higher breathing rate helps minimize respiratory muscle fatigue. Although the adaptation in breathing pattern affects the effectiveness of gas exchange, prevention of muscle fatigue and respiratory arrest requires modification of the breathing pattern (i.e., there is a decrease in tidal volume and an increase in breathing rate). Figure 26-1 illustrates this adaptation in patients at risk for respiratory failure. Respiratory muscle weakness increases the relative load for breathing (inspiratory pressure/maximum inspiratory pressure [PI/PImax] ratio, see Figure 26-1), and this can lead to clinical consequences such as dyspnea, impaired exercise performance, ineffective coughing, respiratory insufficiency, weaning failure, and death. Dysfunction of the respiratory muscles is observed in several conditions such as chronic obstructive pulmonary disease, asthma, cystic fibrosis, neuromuscular disease including spinal cord injury, congestive heart failure, and critical illness. This chapter describes the clinical relevance of respiratory muscle weakness, the assessment and testing of respiratory muscle function, and the application and effectiveness of respiratory muscle training for the conditions above and its role in weaning some patients from mechanical ventilation. Clinically, respiratory muscle strength is measured as PImax and maximum expiratory pressure (PEmax). These pressures are measured using a small cylinder that fits in the patient’s mouth with a circular mouthpiece (Figure 26-2). A small leak in the cylinder (2 mm diameter and 15 mm length) prevents high pressures that could be caused by the contraction of the cheek muscles.2 Standardizing the lung volume at which the pressures are measured is crucial.3 To prevent chest wall and lung recoil pressures from contributing to the pressure generated by the inspiratory muscles, measurements are recorded at functional residual capacity (FRC). This lung volume, however, is difficult to standardize. In clinical practice, PImax is measured from residual volume, whereas PEmax is measured at total lung capacity (TLC). At least five repetitions should be performed. Respiratory muscle testing is described in detail in the American Thoracic Society/European Respiratory Society position statement (2002).4 Several groups of investigators have published norms for PImax and PEmax (Table 26-1).2,7,8 Regardless of the norms used, the standard deviation is typically large. Therefore weakness is not easy to define.11 Inspiratory weakness is defined as a PImax lower than 50% of predicted12 in the presence of clinical signs (e.g., dyspnea, impaired cough, and orthopnea) consistent with reduced respiratory muscle strength. Other methods, such as the sniff maneuver, have been developed as tools to quantify global respiratory muscle function.13 The results of the sniff maneuver have been reported to be highly reliable in children with neuromuscular disease. More invasive methods such as electric or magnetic diaphragm stimulation can provide more accurate and detailed information on diaphragmatic function14 and are useful in the diagnosis of diaphragmatic paresis. For most clinical applications, however, the assessment of inspiratory and expiratory mouth pressures is sufficient. Table 26-1 Reference Values for Maximal Inspiratory and Expiratory Mouth Pressures in Healthy Adults Several tests for assessing respiratory muscle endurance capacity have been described. Most commonly the patient breathes against a submaximal inspiratory load (60% to 75% PImax) for as long as possible.15,16 This test can detect changes in inspiratory muscle endurance after training. Incremental threshold loading, breathing against an incremental load (approximately 5 cm H2O) every 2 minutes, is also reproducible.17 The highest load that can be sustained for two minutes is termed the sustainable pressure and is expressed as a percentage of the maximal load.17,18 Healthy people can usually sustain 70% of the PImax for 2 minutes.18 Johnson and colleagues17 reported large intra-individual variations in this percentage, which tends to decrease with age. The sustainable pressure has been shown to be less than the maximal inspiratory and expiratory pressures in individuals with chronic obstructive pulmonary disease (COPD).19 A third method20–22 is a repetitive maximal inspiratory or expiratory maneuver performed against an occluded airway with a well-defined contraction duration (10 seconds) and relaxation time (5 seconds). The relative decline in maximal pressure after 18 contractions is a measure of the endurance capacity of the respiratory muscles. Comparable to muscle training of the peripheral skeletal muscles, training of the respiratory muscles aims to improve specific characteristics of inspiratory or expiratory muscle contraction force, endurance, or velocity (Table 26-2).23–25 Table 26-2 Because the inspiratory muscles are mainly involved in repetitive contractions with low intensity, training strategies emphasize enhancing inspiratory muscle endurance. Two types of training (i.e. threshold loading [Figure 26-3] and normocapnic hyperpnea [NCH] [Figure 26-4]) are currently practiced. During NCH, the patient is asked to breathe at a high proportion (>60%) of the maximal voluntary ventilation for 15 to 20 minutes.23,26 In the past, the equipment used for this type of training was complicated, but recently a simpler, partial rebreathing system has been developed.27 During inspiratory resistive breathing the patient inhales through a mouthpiece with an adapter fitted with an adjustable diameter. This resistance is flow-dependent. Adequate training intensity is achieved only with feedback of the target pressure if flow and pressure are tightly coupled.28 Recently, a flow-independent resistance has been developed, the so-called threshold loading valve, a valve that opens at a critical pressure.29,30 Training intensity varies across studies, from as high as maximal sustained inspiratory (Müller) maneuvers31 to 50% to 80% PImax16,32–34 to a low intensity of 30% PImax.34–37 All these studies carefully controlled the target pressure or the threshold loading during training.30 Threshold loading has the advantage of being independent of inspiratory flow rate30 but requires a build-up of negative pressure before flow is initiated; hence it is inertive in nature. The fact that threshold loading enhances velocity of inspiratory muscle shortening38 could provide additional benefit because this shortens inspiratory time and increases time for exhalation and relaxation. Increased relaxation time may prevent the development of muscle fatigue in patients who are at risk. In addition, shortening inspiratory time will increase expiratory time, thus reducing dynamic hyperinflation, which is an important advantage in patients with COPD. Explosive expiratory maneuvers and low-intensity contractions of the abdominal muscles are similar to those involved in coughing, the Valsalva maneuver, and exercise. Consequently, training parameters for expiratory muscle training can be either high-intensity strength training or moderate- to low-intensity endurance training. An example of the parameters for endurance expiratory muscle training is 30 minutes of continuous training at 15% to 45% of PEmax.39 An example of strength training parameters is 15 Valsalva maneuvers at 60% of PEmax.40 Both training programs can be implemented using expiratory resistance at the mouth, such as threshold loading.40,41 Diaphragm fatigue can occur during sustained high-intensity exercise.42,43 Several studies have shown that unloading respiratory muscles (by using low-density gas mixtures or mechanical ventilation) can lead to an increase in exercise performance.44,45 In athletes, heavy (but not moderate) respiratory muscle work has an impact on whole body exercise performance by affecting limb blood flow and limb muscle fatigue during heavy exercise.46,47 One mechanism to explain these improvements in exercise performance is the “respiratory muscle metaboreflex” (Figure 26-5).47 Therefore a rational basis exists for improving the strength and endurance of the respiratory muscles in order to improve exercise performance. In 14 competitive rowers, inspiratory muscle training (IMT) significantly improved PImax and performance on a 5000-meter trial compared with a placebo control group.48 A small but significant decrease in swimming time needed to cover 100 meters and 200 meters was observed after 6 weeks of IMT compared with a placebo control group.49 After following 5 weeks of respiratory muscle endurance training (RMET), nine competitive cyclists had a 25 seconds (+2%) improvement on an 8-km trial. No differences were founded in peak work rate or maximal exercise capacity ( Respiratory muscle weakness is often observed in patients with chronic obstructive pulmonary disease (COPD).54–58 Adaptation of the diaphragm results in greater fatigue resistance and improved muscle function.59,60 The diaphragm is remodeled in part by the transformation of fast fiber types to slow fiber types.61,62 Despite these adaptations, both functional inspiratory muscle strength55 and endurance56 remain compromised in patients with COPD and contribute to hypercapnia,63 dyspnea,64,65 nocturnal oxygen desaturation,33 and reduced walking distance.66 During exercise, patients with COPD use a larger proportion of their maximal inspiratory pressure than healthy people.67 This pattern of breathing is closely related to dyspnea during exercise67 and may induce respiratory muscle fatigue and probably limits exercise capacity. Another mechanism involved in the potential role of respiratory muscles in exercise limitation is the respiratory muscle metaboreflex (see Figure 26-5). Inspiratory muscles should become more fatigue-resistant by increasing their work capacity and should consume a smaller fraction of the total cardiac output during exercise, which in turn, should be available for the working muscles during exercise. In patients with COPD, diaphragmatic fatigue after exercise has been observed in only a small number of patients.11,68 However, this might be related to the insufficient length of the exercise protocols and the absence of inspiratory muscle weakness in the subjects evaluated. Improved limb muscle blood flow after IMT has been observed in patients with chronic heart failure69–71 but has not yet been studied in patients with COPD. Reductions in dynamic hyperinflation and dyspnea during exercise after IMT have also been proposed as mechanisms linking inspiratory muscle capacity to whole body endurance capacity; thus further study is needed.72 Compelling evidence suggests that breathing against an inspiratory load increases both maximal inspiratory pressure16,28,32–37,73 and endurance of the inspiratory muscles.28,33,34,73 Respiratory muscle training has been reported to produce hypertrophy of predominantly type I and IIA fibers in the diaphragms of hamsters.74,75 The proportion of type I fibers and size of type II fibers in the external intercostals after IMT has been recently reported to increase in a study of patients with COPD.76 Dyspnea36,37,77 and nocturnal desaturation time33 also decreased, while exercise performance tended to improve (Table 26-3).78,79 In addition to exercise training, IMT can improve exercise capacity more than exercise training alone.16,32,35,37 Based on systematic reviews with meta-analyses, IMT can improve inspiratory muscle strength and endurance, functional exercise capacity, and quality of life while also decreasing dyspnea.78,79 The addition of IMT to a general exercise training program improved PImax and tended to improve the exercise performance of patients with inspiratory muscle weakness (PImax < 60 cm H2O).78,79 Long-term effects were shown for exercise performance and dyspnea in patients with COPD who continued performing their training program three times per week at high training intensity (60% PImax).80 NCH was applied in one randomized controlled trial and resulted in enhanced respiratory muscle endurance and exercise capacity as well as quality of life in patients with COPD.26 Inspiratory muscle endurance training was shown to be less effective than respiratory muscle strength training.79 Table 26-3 Effect Size of Inspiratory Muscle Training Based on Meta-Analysis (n = 32) From Gosselink R, De Vos J, van den Heuvel SP, et al: Impact of inspiratory muscle training in patients with COPD: What is the evidence? Eur Respir J 2011;37:416-425, 2011. Respiratory muscle weakness is not frequently observed in patients with asthma.80–82 Although some studies report a moderate reduction in inspiratory muscle strength,81 other studies have not found inspiratory muscle strength to be affected.20,56 Inspiratory muscle endurance has been shown to be increased in people with asthma20 but reduced in those who are steroid dependent.56 In patients with asthma, dyspnea has been observed to be greater in women than in men, resulting in their greater need for beta-2 agonists. This may reflect sex differences in inspiratory muscle strength.80 IMT has been studied in people with asthma, and evidence from randomized trials supports that, in addition to improvements in inspiratory muscle strength, dyspnea and beta-2 agonist use was reduced in those with high dyspnea and high use of beta-2 agonists,83 especially among women.80 A Cochrane review, however, concluded that the evidence supporting a role for IMT for people with asthma was inconclusive.84 Reports on the inspiratory muscle strength in people with cystic fibrosis (CF) have also been contradictory. Some have shown that inspiratory muscle strength is decreased,85–88 whereas others have shown that it is normal89,90 and others have shown it is supranormal.91–93
Respiratory Muscle Training
Respiratory Muscle Assessment
Respiratory Muscle Strength Testing
Reference
PImax (cm H2O)
PEmax (cm H2O)
Black and Hyatt (1969)2
M
F
124 ± 22
87 ± 16
233 ± 42
152 ± 27
Rinqvist (1966)5
M
F
130 ± 32
98 ± 25
237 ± 46
165 ± 30
Leech et al (1983)6
M
F
114 ± 36
71 ± 27
154 ± 82
94 ± 33
Rochester and Arora (1983)7
M
F
127 ± 28
91 ± 25
216 ± 41
138 ± 39
Wilson et al (1984)8
M
F
106 ± 31
73 ± 22
148 ± 17
93 ± 17
Vincken et al (1987)9
M
F
105 ± 25
71 ± 23
140 ± 38
89 ± 24
Bruschi et al (1992)10
M
F
120 ± 37
84 ± 30
140 ± 30
95 ± 20
Respiratory Muscle Endurance Testing
Respiratory Muscle Training Methods
IMT
RMET (Voluntary Isocapnic Hyperpnea)
Type
Strength
Endurance
Duration
15 minutes, twice daily,
30 minutes, 6-12 weeks
Frequency
5-7x per week
5x per week
Intensity
30-50%PImax with individual incremental load, weekly control of load/technique
VE = 50-60% MVV, breathing frequency 50-60/min
Inspiratory Muscle Training


Expiratory Muscle Training
Respiratory Muscle Training in Health
 ).50 Leddy and colleagues (2007)51 reported a 4% decrease in time on a 4-mile run after 4 weeks of RMET. All these small improvements in exercise performance are also practical and relevant since small differences in athletes’ performance can be the difference between winning and losing a race. On the other hand, several studies in endurance athletes observed no differences in maximal exercise capacity, other than an increase in respiratory muscle strength and endurance.52,53
).50 Leddy and colleagues (2007)51 reported a 4% decrease in time on a 4-mile run after 4 weeks of RMET. All these small improvements in exercise performance are also practical and relevant since small differences in athletes’ performance can be the difference between winning and losing a race. On the other hand, several studies in endurance athletes observed no differences in maximal exercise capacity, other than an increase in respiratory muscle strength and endurance.52,53
Respiratory Muscle Training in Disease
Chronic Obstructive Pulmonary Disease
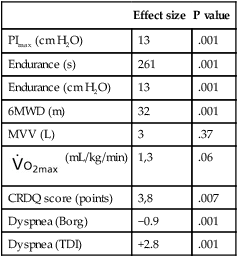
Effect size
P value
PImax (cm H2O)
13
.001
Endurance (s)
261
.001
Endurance (cm H2O)
13
.001
6MWD (m)
32
.001
MVV (L)
3
.37
 (mL/kg/min)
(mL/kg/min)
1,3
.06
CRDQ score (points)
3,8
.007
Dyspnea (Borg)
−0.9
.001
Dyspnea (TDI)
+2.8
.001
Asthma
Cystic Fibrosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Respiratory Muscle Training
 , maximal oxygen uptake capacity; CRDQ, chronic respiratory disease questionnaire; Borg, scale of breathlessness; TDI, total dyspnea index.
, maximal oxygen uptake capacity; CRDQ, chronic respiratory disease questionnaire; Borg, scale of breathlessness; TDI, total dyspnea index.