Increased uric acid (UA) is strongly linked to cardiovascular disease. However, the independent role of UA is still debated because it is associated with several cardiovascular risk factors including obesity and metabolic syndrome. This study assessed the association of UA with increased high-sensitivity C-reactive protein (hs-CRP), increased ratio of triglyceride to high-density lipoprotein cholesterol (TG/HDL), sonographically detected hepatic steatosis, and their clustering in the presence and absence of obesity and metabolic syndrome. We evaluated 3,518 employed subjects without clinical cardiovascular disease from November 2008 through July 2010. Prevalence of hs-CRP ≥3 mg/L was 19%, that of TG/HDL ≥3 was 44%, and that of hepatic steatosis was 43%. In multivariable logistic regression after adjusting for traditional cardiovascular risk factors and confounders, highest versus lowest UA quartile was associated with hs-CRP ≥3 mg/L (odds ratio [OR] 1.52, 95% confidence interval [CI] 1.01 to 2.28, p = 0.04), TG/HDL ≥3 (OR 3.29, 95% CI 2.36 to 4.60, p <0.001), and hepatic steatosis (OR 3.10, 95% CI 2.22 to 4.32, p <0.001) independently of obesity and metabolic syndrome. Association of UA with hs-CRP ≥3 mg/L became nonsignificant in analyses stratified by obesity. Ascending UA quartiles compared to the lowest UA quartile demonstrated a graded increase in the odds of having 2 or 3 of these risk conditions and a successive decrease in the odds of having none. In conclusion, high UA levels were associated with increased TG/HDL and hepatic steatosis independently of metabolic syndrome and obesity and with increased hs-CRP independently of metabolic syndrome.
Increased serum uric acid (UA), the end product of purine metabolism, is strongly associated with cardiovascular disease (CVD) including coronary heart disease and stroke. However, the underlying mechanism linking hyperuricemia to CVD risk is unclear. In particular, controversy exists about whether UA is a causative risk factor or merely a marker of other proatherogenic processes. Some studies have found that the association between UA and cardiometabolic risk factors is largely decreased or eliminated after adjusting for body mass index and metabolic syndrome components. The objective of this study was to investigate the independent relation between UA and early markers of cardiometabolic risk. We evaluated the association of UA with systemic inflammation (measured by high-sensitivity C-reactive protein [hs-CRP]), dyslipidemia of insulin resistance (measured by the ratio of triglyceride to high-density lipoprotein cholesterol [TG/HDL]), and hepatic steatosis (measured by ultrasound) in the presence and absence of obesity and metabolic syndrome in a healthy Brazilian population.
Methods
The study population consisted of predominantly Caucasian 21- to 85-year-old men and women free of clinical CVD who underwent a required employer-sponsored health examination from November 2008 through July 2010 at the Preventive Medicine Center of the Hospital Israelita Albert Einstein in São Paulo, Brazil. The local institutional review board approved the study and granted a waiver for informed consent. The 3,518 subjects included in this analysis had complete information on hs-CRP, TG/HDL, and hepatic steatosis. Participants missing information on these conditions (n = 678) were more likely to be older men taking lipid-lowering medications with lower low-density lipoprotein cholesterol and higher physical activity levels. None of the participants reported using xanthine oxidase inhibitors or having gout.
Demographic, lifestyle, and medical history information was gathered by questionnaire. Alcohol use was quantified by the Alcohol Use Disorders Identification Test as a numerical score, and physical activity was categorized by the International Physical Activity Questionnaire as none, low, moderate, or high. Hypertension was identified by previous physician diagnosis, use of blood pressure-lowering medications, or mean blood pressure >140/90 mm Hg, which was calculated from 3 different measurements that followed American Heart Association guidelines. Waist circumference was assessed with a tape measure placed parallel to the floor around the smallest diameter between the iliac crest and the costal margin. Obesity was defined as body mass index ≥30 kg/m 2 or waist circumference >88 cm in women and >102 cm in men with body mass index >25 kg/m 2 .
Laboratory tests were conducted using fasting blood samples. Serum UA, TG, total cholesterol, and plasma glucose levels were measured with enzymatic colorimetric assays on a Vitros automated platform (Johnson & Johnson Clinical Diagnostics). HDL cholesterol was obtained using a precipitation method, and low-density lipoprotein cholesterol was calculated by the Friedewald equation for TGs ≤400 mg/dl. All tests were performed at the central laboratory of the Albert Einstein Hospital. Glomerular filtration rate was estimated by the Chronic Kidney Disease Epidemiology Collaboration equation. Metabolic syndrome was defined by International Diabetes Federation criteria. Participants were identified as having metabolic syndrome if they had abdominal obesity (waist circumference >88 cm in women or >102 cm in men or body mass index >30 kg/m 2 ) and ≥2 of the following factors: hypertriglyceridemia (≥150 mg/dl or lipid-lowering medication), low HDL cholesterol (<40 mg/dl in men and <50 mg/dl in women), high blood pressure (≥130/85 mm Hg or antihypertensive medication), or hyperglycemia (fasting blood glucose ≥100 mg/dl).
hs-CRP was assessed by immunonephelometry (Dade-Behring, Newark, Delaware). hs-CRP ≥3 mg/L was defined as increased based on prospective studies that showed increased CV risk at this level. The previously established cut point of TG/HDL ≥3 was used to identify insulin resistance. TG/HDL is an acceptable marker of insulin resistance in Caucasians, with an area under the receiver operating characteristic curve of 0.770 for predicting the homeostasis model assessment of insulin resistance. Abdominal ultrasounds, which have 100% sensitivity for detecting >33% liver fat, were obtained after a minimum of 6 hours of fasting. Images were obtained with an Acuson XP-10 scanner (Acuson, Mountain View, California) and read by 2 board-certified radiologists who were blinded to laboratory test data. Hepatic steatosis was defined as the presence of a bright liver with evident contrast between hepatic and renal parenchyma.
Statistical analyses were performed using STATA 12 (STATA Corp., College Station, Texas). Age, gender, clinical diagnoses, medication use, and risk factors were compared across UA quartiles using 1-way analysis of variance for continuous variables and Pearson chi-square test for categorical variables. Median values of skewed variables were compared using the Kruskal–Wallis test. Multivariable linear regression analyses were performed to assess associations of natural log-transformed hs-CRP and natural log-transformed TG/HDL as separate dependent variables with continuous UA as the independent variable. Multivariable logistic regression analyses were used to characterize associations of hs-CRP ≥3 mg/L, TG/HDL ≥3, and hepatic steatosis with continuous UA and UA quartiles. Subgroup analyses were conducted to investigate the odds ratio (OR) of each outcome in the fourth versus first UA quartile in the presence and absence of obesity and metabolic syndrome. To evaluate the relation of UA with increased hs-CRP, increased TG/HDL, and hepatic steatosis simultaneously, multivariable logistic regression was used to assess the association of UA with 0, 1, 2, or 3 of these conditions.
Results
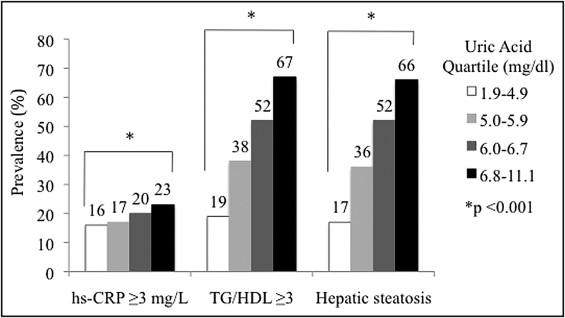
CV characteristics of the study population of 3,518 subjects (mean age 48 ± 8 years, 81% men) were stratified by UA quartile ( Table 1 ). Participants in the fourth versus first UA quartile were older and more likely to be men. Subjects in higher UA quartiles demonstrated a graded increase in systolic blood pressure, low-density lipoprotein cholesterol, TGs, body mass index, waist circumference, and fasting glucose and a graded decrease in HDL cholesterol and physical activity. Increasing UA quartiles also displayed a successive increase in prevalence of hypertension, obesity, and metabolic syndrome. Overall, ascending UA quartiles exhibited a significant increase in prevalence of hs-CRP ≥3 mg/L, TG/HDL ≥3, and hepatic steatosis ( Figure 1 ).
| Characteristics | UA Quartiles (mg/dl) | p Value | |||
|---|---|---|---|---|---|
| 1.9–4.9 | 5.0–5.8 | 5.9–6.7 | 6.8–11.1 | ||
| (n = 920) | (n = 843) | (n = 886) | (n = 869) | ||
| Age (years) | 47 ± 8 | 49 ± 8 | 49 ± 7 | 49 ± 8 | 0.0005 |
| Men | 403 (44%) | 738 (88%) | 847 (96%) | 862 (99%) | <0.0001 |
| Systolic blood pressure (mm Hg) | 114 ± 13 | 121 ± 12 | 123 ± 12 | 125 ± 14 | <0.0001 |
| Hypertension | 83 (9%) | 141 (17%) | 171 (19%) | 223 (26%) | <0.0001 |
| Low-density lipoprotein cholesterol (mg/dl) | 126 ± 32 | 133 ± 33 | 136 ± 33 | 139 ± 35 | <0.0001 |
| High-density lipoprotein cholesterol (mg/dl) | 55 ± 14 | 47 ± 12 | 45 ± 11 | 43 ± 11 | <0.0001 |
| Triglycerides (mg/dl) | 92 (71–126) | 116 (88–157) | 131 (97–182) | 163 (116–223) | <0.0001 |
| Waist circumference (cm) | 84 ± 11 | 94 ± 10 | 97 ± 10 | 100 ± 10 | <0.0001 |
| Body mass index (kg/m 2 ) | 24 ± 3 | 27 ± 3 | 27 ± 4 | 29 ± 4 | <0.0001 |
| Obesity ⁎ | 130 (14%) | 219 (26%) | 289 (33%) | 371 (43%) | <0.0001 |
| Fasting glucose (mg/dl) | 86 ± 8 | 90 ± 12 | 93 ± 11 | 94 ± 10 | <0.0001 |
| Metabolic syndrome | 80 (9%) | 174 (21%) | 253 (29%) | 388 (45%) | <0.0001 |
| Antihypertensive medications | 83 (9%) | 134 (16%) | 167 (19%) | 225 (26%) | <0.0001 |
| Lipid-lowering medications | 81 (9%) | 98 (12%) | 109 (12%) | 108 (12%) | 0.050 |
| Hypoglycemic medications | 1 (0%) | 8 (1%) | 13 (1%) | 13 (2%) | 0.009 |
| Glomerular filtration rate (ml/min/1.73 m 2 ) | 104 ± 12 | 101 ± 12 | 99 ± 12 | 96 ± 14 | <0.0001 |
| Current smokers | 75 (8%) | 79 (9%) | 82 (9%) | 79 (9%) | 0.793 |
| Physical activity | <0.0001 | ||||
| Sedentary | 151 (20%) | 152 (21%) | 175 (23%) | 189 (26%) | |
| Little activity | 221 (29%) | 226 (32%) | 279 (27%) | 269 (37%) | |
| Active | 275 (36%) | 259 (36%) | 244 (32%) | 228 (31%) | |
| Very active | 108 (14%) | 76 (11%) | 59 (8%) | 45 (6%) | |
⁎ Obesity is defined as body mass index ≥30 kg/m 2 or waist circumference >88 cm in women or >102 cm in men if body mass index >25 kg/m 2 .
In linear regression analyses, continuous UA was significantly associated with natural log-transformed hs-CRP and natural log-transformed TG/HDL even after controlling for traditional CVD risk factors and confounders including obesity and metabolic syndrome ( Table 2 ). In logistic regression analyses, continuous UA was significantly associated with hs-CRP ≥3 mg/L, TG/HDL ≥3, and hepatic steatosis. After adjusting for CVD risk factors, confounders, obesity, and metabolic syndrome, every 1-SD (1.41 mg/dl) increase in UA was associated with a significantly greater odds of increased hs-CRP (OR 1.56, 95% confidence interval [CI] 1.41 to 1.73, p = 0.04), increased TG/HDL (OR 2.12, 95% CI 1.93 to 2.32, p <0.001), and hepatic steatosis (OR 1.99, 95% CI 1.81 to 2.18, p <0.001).
| Outcome | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| Δ per SD UA (95% CI) | p Value | Δ per SD UA (95% CI) | p Value | Δ per SD UA (95% CI) | p Value | |
| Natural log-transformed high-sensitivity C-reactive protein | 0.15 (0.12–0.19) | <0.001 | 0.22 (0.17–0.27) | <0.001 | 0.12 (0.07–0.18) | <0.001 |
| Natural log-transformed triglyceride/high-density lipoprotein cholesterol | 0.30 (0.28–0.32) | <0.001 | 0.22 (0.19–0.25) | <0.001 | 0.15 (0.12–0.18) | <0.001 |
Each ascending UA quartile compared to the lowest UA quartile demonstrated a graded increase in the odds of hs-CRP ≥3 mg/L, TG/HDL ≥3, and hepatic steatosis in hierarchical logistic regression models ( Table 3 ). After adjusting for traditional CVD risk factors, obesity, and metabolic syndrome, the second, third, and fourth UA quartiles compared to the first were each significantly associated with increased odds of increased TG/HDL and hepatic steatosis, and the highest versus lowest UA quartile had a significantly greater odds of increased hs-CRP. In the fully adjusted model, p values for linear trend across UA quartiles were <0.05 for increased hs-CRP and <0.001 for increased TG/HDL and hepatic steatosis.
| Outcome | UA Quartile | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | ||
| High-sensitivity C-reactive protein ≥3 mg/L | 4 | 1.59 (1.25–2.02) | <0.001 | 2.26 (1.50–3.31) | <0.001 | 1.52 (1.01–2.28) | 0.04 |
| 3 | 1.33 (1.04–1.69) | 0.02 | 1.72 (1.17–2.52) | 0.01 | 1.32 (0.90–1.94) | 0.15 | |
| 2 | 1.10 (0.85–1.42) | 0.46 | 1.37 (0.95–1.97) | 0.09 | 1.11 (0.77–1.59) | 0.57 | |
| 1 | 1 (reference) | – | 1 (reference) | – | 1 (reference) | – | |
| Triglyceride/high-density lipoprotein cholesterol ≥3 | 4 | 8.39 (6.76–10.42) | <0.001 | 4.83 (3.56–6.55) | <0.001 | 3.29 (2.36–4.60) | <0.001 |
| 3 | 4.43 (3.59–5.46) | <0.001 | 2.58 (1.93–3.43) | <0.001 | 2.14 (1.57–2.91) | <0.001 | |
| 2 | 2.57 (2.08–3.19) | <0.001 | 1.70 (1.28–2.25) | <0.001 | 1.44 (1.06–1.96) | 0.02 | |
| 1 | 1 (reference) | – | 1 (reference) | – | 1 (reference) | – | |
| Hepatic steatosis | 4 | 9.38 (7.52–11.71) | <0.001 | 5.16 (3.75–7.10) | <0.001 | 3.10 (2.22–4.32) | <0.001 |
| 3 | 5.26 (4.23–6.52) | <0.001 | 3.29 (2.44–4.45) | <0.001 | 2.46 (1.80–3.36) | <0.001 | |
| 2 | 2.69 (2.16–3.36) | <0.001 | 1.85 (1.38–2.49) | <0.001 | 1.43 (1.06–1.93) | 0.02 | |
| 1 | 1 (reference) | – | 1 (reference) | – | 1 (reference) | – | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


