Microalbuminuria is one of the strongest predictors of both adverse renal and cardiovascular disease (CVD) outcomes in patients with type 2 diabetes mellitus. Although measurement of urinary albumin excretion (UAE) is widely recommended, limited data are available to suggest that reducing UAE translates into a reduction in long-term cardiovascular mortality, particularly among patients without overt nephropathy, who constitute most patients with type 2 diabetes worldwide. We assessed whether changes in the UAE at 1 year were associated with cardiovascular mortality in 393 patients with hypertension and type 2 diabetes during a 10-year period. On univariate analysis, CVD history, age, diabetes duration, and change in UAE at 1 year were associated with cardiovascular mortality risk (hazard ratio 2.60 for those with CVD history, 95% confidence interval [CI] 1.47 to 4.62; hazard ratio 1.59 per 10 years of diabetes duration, 95% CI 1.12 to 2.25; and hazard ratio 1.49 per log UAE increase, 95% CI 1.13 to 1.96). In a stepwise Cox regression model that included baseline UAE and CVD history, the 10-year predicted mortality of those with a decrease in UAE of 2 logs at 1 year was 4.7% (95% CI 1.4% to 7.8%). For those with an increase in UAE of 2 logs at 1 year, it was 24.5% (95% CI 10.1% to 36.5%). In conclusion, these data support current guideline recommendations to screen for UAE in all patients with type 2 diabetes, even in the absence of nephropathy, and suggest that serial UAE measurements even after the initiation of antihypertensive therapy has prognostic value independent of traditional cardiovascular risk factors.
Little evidence exists examining the association between changes in urinary albumin excretion (UAE) and cardiovascular outcomes. In patients with overt albuminuria enrolled in the Reduction in Endpoints in Non–insulin dependent diabetes mellitus with the Angiotensin II Antagonist Losartan (RENAAL), a post hoc analysis demonstrated that a reduction in UAE provided cardiovascular protection. In that study, every 50% decrease in albuminuria reduced the risk of cardiovascular events by 18% (95% confidence interval [CI] 9% to 25%) and heart failure by 27% (95% CI 14% to 38%). Among diabetic patients with normo- or microalbuminuria, who constitute most patients with type 2 diabetes worldwide, no study to date has shown a significant reduction in cardiovascular mortality associated with a reduction in UAE. We, therefore, examined the association between the 1-year change from baseline in UAE with cardiovascular mortality during a 10-year period across a spectrum of patients with hypertension and type 2 diabetes with baseline normo-, micro-, and overt albuminuria.
Methods
We performed a longitudinal investigation of the hypertensive cohort of the Appropriate Blood Pressure Control in Diabetes (ABCD) trial to evaluate the association between the 1-year change in UAE from baseline and cardiovascular mortality after 10 years of follow-up from June 19, 1991 to October 21, 2003. The ABCD trial constituted 2 sequentially linked, randomized controlled studies. The original ABCD investigation evaluated the effects of intensive versus moderate diastolic blood pressure control in a normotensive (n = 480) and a hypertensive (n = 470) cohort during a 5-year follow-up period. After the termination of the ABCD study in 1998, continued study participation was possible in a second trial using valsartan as the primary antihypertensive medication. The original randomization into intensive or moderate blood pressure control was maintained for an additional 5 years, resulting in a 10-year period for longitudinal follow-up.
The details of the study design have been previously reported. In brief, the subjects aged 40 to 74 years were identified from administrative and pharmacy lists among participating healthcare systems in the Denver metropolitan area. All patients had type 2 diabetes according to the World Health Organization criteria. Hypertensive subjects, who constituted the present analysis cohort, had a diastolic blood pressure >90 mm Hg at enrollment and were not taking any antihypertensive medications at randomization. Patients were excluded if they had a known allergy to dihydropyridine calcium channel antagonists or angiotensin-converting enzyme (ACE) inhibitors, had experienced myocardial infarction, unstable angina pectoris, or cerebral vascular accident within the previous 6 months, or had undergone coronary artery bypass surgery within the previous 3 months. Additional exclusions were New York Heart Association class III to IV congestive heart failure, an absolute need for ACE inhibitors or calcium channel antagonists, chronic dialysis, and/or a serum creatinine >3 mg/dl (265.2 μmol/L).
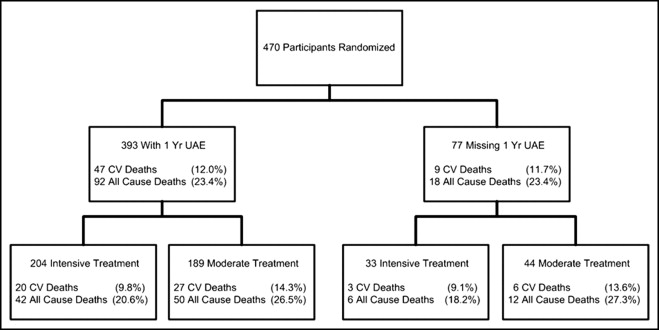
Normoalbuminuria was defined as <20 μg/min (30 mg/24 hours), microalbuminuria as 20 to 200 μg/min (30 to 300 mg/24 hours), and overt albuminuria as >200 μg/min (>300 mg/24 hours). UAE was measured using radioimmunoassay techniques from 24-hour and overnight collections. At baseline, the stage of UAE (normoalbuminuria, microalbuminuria, and overt albuminuria) was classified using the median of a single 24-hour collection and 2 overnight collections. The follow-up 24-hour UAE was measured from 24-hour collections annually or by overnight collections measured every 6 months, starting 3 months after randomization. Patients were included in the analysis population if they had both a baseline and 1-year measurement (±6 months) of UAE (n = 393; Figure 1 ).
An independent clinical end point committee unaware of the study intervention arms adjudicated all deaths. Cardiovascular mortality encompassed sudden or arrhythmia deaths, progressive heart failure fatalities, fatal myocardial infarction, fatal cerebral vascular accidents, and ruptured aortic aneurysm. Of 189 patients who did not participate in the continuation study, vital status was obtained at the end of study by obtaining the medical and federal death records or by telephone interview. Vital status was obtained for 375 patients (95.4%) at 10 years.
Because UAE is positively skewed, the baseline UAE was defined as the median urinary excretion rate of a single 24-hour collection and 2 overnight collections. The 1-year UAE was taken as the collection closest to the 1-year postrandomization date within a window of ±6 months. The analysis population included 393 patients for whom a 1-year change in UAE could be calculated. The baseline and 1-year UAEs were log transformed before calculating the 1-year change from baseline. The distribution of continuous variables for the analysis population was compared to the excluded population using 2-sample t tests, and categorical variables were compared using the chi-square test.
After the initial 5 years of follow-up, patients could continue participation according to their original randomization assignment of intensive or moderate blood pressure control. For most patients, an interim period occurred between termination of the initial 5-year period and continuation of the study (median 18.1 months). Accordingly, a time-varying participation indicator was created for each patient in 3-month windows to account for the period between the initial 5 years of follow-up and continuation of participation when the patient was not actively being monitored.
The univariate associations between the baseline demographics, baseline risk factors, 1-year change in log-transformed UAE from baseline, and study design variables with cardiovascular mortality were evaluated using Cox proportional hazards models. The baseline demographics included gender, age, and race/ethnicity. The baseline risk factors included cardiovascular disease (CVD) history, hypertension duration, diabetes duration, smoking status, systolic and diastolic blood pressure, body mass index, hemoglobin A1c, total cholesterol, and baseline UAE category (normo-, micro-, and overt albuminuria). The study design variables included blood pressure control (intensive vs moderate), initial study drug (enalapril vs nisoldipine), and the time-varying participation indicator. The assumption of proportional hazards was assessed individually for each of the covariates. The assumption of linearity was assessed for each continuous covariate by testing the quadratic and cubic term in these univariate Cox proportional hazards models.
All covariates tested univariately were included in a multiple Cox proportional hazards model. Stepwise selection, which included a series of steps to add and subtract covariates from the model, was used to find a model with the most parsimonious set of covariates with statistical significance. This method was used to help identify the covariates with the strongest relation to cardiovascular mortality at 10 years at the 5% significance level. All tests were 2-sided and evaluated at the 5% level of significance. Analyses were conducted using SAS software, version 9 or higher (SAS Institute, Cary, North Carolina).
Results
Of the 470 patients with hypertension and type 2 diabetes randomized, 393 (83.6%) had the UAE measured at both baseline and 1 year of follow-up ( Figure 1 ). These subjects constituted our analysis cohort and had similar baseline characteristics and follow-up mortality (data not shown) compared to the 77 subjects without the 1-year change in UAE data. However, the analysis cohort had a shorter diabetes duration, lower baseline systolic blood pressure, lower baseline serum creatinine and UAE, and greater creatinine clearance than the 77 subjects without the 1-year change in UAE data (all p <0.05). The characteristics of the analysis cohort stratified by intensive and moderate blood pressure treatment cohorts are listed in Table 1 . The mean age of the overall population was 57.8 years, and the mean blood pressure was 154/98 mm Hg. During the 10-year follow-up period, no differences were seen in the rate of all-cause or cardiovascular mortality between the analysis cohort and the subjects without the 1-year change in UAE data.
| Characteristic | Blood Pressure Control | ||
|---|---|---|---|
| Intensive (n = 204) | Moderate (n = 189) | All Patients (n = 393) | |
| Age (years) | 58.0 ± 8.4 | 57.5 ± 8.3 | 57.8 ± 8.3 |
| Men | 140 (68.6%) | 132 (69.8%) | 272 (69.2%) |
| Diabetes duration (years) | 8.5 ± 7.0 | 8.1 ± 6.4 | 8.3 ± 6.7 |
| Hypertension duration (years) | 11.7 ± 10.0 | 11.1 ± 9.6 | 11.4 ± 9.8 |
| Cardiovascular disease | 64 (31.5%) | 54 (28.6%) | 118 (30.1%) |
| Hemoglobin A1c (%) | 11.5 ± 3.2 | 11.5 ± 3.1 | 11.5 ± 3.1 |
| Total cholesterol (mg/dl) | 215.2 ± 49.3 | 219.4 ± 63.0 | 217.3 ± 56.3 |
| Body mass index (kg/m 2 ) | 31.6 ± 5.0 | 31.4 ± 6.0 | 31.5 ± 5.5 |
| Smoking status (%) | |||
| Never | 75 (36.8%) | 68 (36.0%) | 143 (36.4%) |
| Past | 103 (50.5%) | 90 (47.6%) | 193 (49.1%) |
| Current | 26 (12.7%) | 31 (16.4%) | 57 (14.5%) |
| Systolic blood pressure at randomization (mm Hg) | 156.2 ± 15.5 | 151.7 ± 15.8 | 154.0 ± 15.8 |
| Diastolic blood pressure at randomization (mm Hg) | 98.1 ± 6.8 | 97.3 ± 6.1 | 97.7 ± 6.5 |
| Education completed (years) | 13.3 ± 2.9 | 13.8 ± 2.4 | 13.5 ± 2.7 |
| Race/ethnicity | |||
| Non-Hispanic white | 132 (64.7%) | 129 (68.3%) | 261 (66.4%) |
| Black | 29 (14.2%) | 32 (16.9%) | 61 (15.5%) |
| Hispanic | 35 (17.2%) | 24 (12.7%) | 59 (15.0%) |
| Other | 8 (3.9%) | 4 (2.1%) | 12 (3.1%) |
| Serum creatinine (mg/dl) | 1.1 ± 0.2 | 1.1 ± 0.2 | 1.1 ± 0.2 |
| Baseline log urinary albumin excretion | 3.4 ± 1.9 | 3.2 ± 1.8 | 3.3 ± 1.9 |
| Creatinine clearance (ml/min/1.73 m 2 ) | 84.0 ± 24.6 | 90.2 ± 48.4 | 87.0 ± 38.1 |
| 1-Year change from baseline | |||
| Log urinary albumin excretion | −0.30 (0.99) | −0.07 (0.91) | −0.18 (0.96) |
| Systolic blood pressure | −24.4 (18.2) | −15.5 (17.0) | −20.2 (18.2) |
| Diastolic blood pressure | −17.3 (9.3) | −10.5 (8.3) | −14.0 (9.4) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


