Coronary artery dominance influences the amount and anatomic location of myocardium that is perfused by the left or right coronary circulation. However, it is unknown whether coronary artery dominance also influences the distribution of coronary blood flow volume. The aim of this study was to evaluate volumetric coronary blood flow in 1,322 vessels from 496 patients in the Prediction of Progression of Coronary Artery Disease and Clinical Outcomes Using Vascular Profiling of Endothelial Shear Stress and Arterial Wall Morphology (PREDICTION) study. Patients were divided into 2 groups (right-dominant and left-dominant or balanced circulation). Coronary blood flow volume was calculated by coronary segment volume measurement using angiography and intravascular ultrasound and the contrast transit time through the segment. Coronary blood flow in the left circumflex coronary artery was significantly higher in left-dominant or balanced circulation than in right-dominant circulation (113 ± 43 vs 72 ± 37 ml/min, p <0.001), whereas flow in the right coronary artery was significantly lower in left-dominant or balanced circulation than in right-dominant circulation (56 ± 40 vs 113 ± 49 ml/min, p = 0.003). There was no significant difference in the left anterior descending coronary artery. In conclusion, coronary artery dominance has an impact on coronary blood flow volume in the left circumflex and right coronary arteries but not in the left anterior descending coronary artery. These findings suggest that the extent of myocardial perfusion area is associated with coronary blood flow volume.
Measurement of blood flow volume in human coronary arteries to obtain a better understanding of coronary physiology has been challenging. Although numerous methodologies have been proposed during the past several decades, they have not yet been established in clinical practice. Recent studies have reported direct volumetric blood flow measurement using Doppler-based methods or thermodilution techniques, but these studies were limited to validation of the techniques. There have been no large-sample investigations applying volumetric coronary blood flow measurements in a clinical setting. Left ventricular myocardial perfusion patterns are strongly affected by coronary artery dominance. Although the dominant artery generally supplies a substantial area of left ventricular myocardium, no data exist as to whether coronary artery dominance influences the coronary artery blood flow. The purpose of this investigation was to determine whether coronary blood flow volume is different according to coronary artery dominance by measuring coronary blood flow volume at rest selectively using vascular profiling (VP).
Methods
We used a large sample of patients enrolled in the Prediction of Progression of Coronary Artery Disease and Clinical Outcomes Using Vascular Profiling of Endothelial Shear Stress and Arterial Wall Morphology (PREDICTION) study, a prospective, multicenter study investigating the role of endothelial shear stress and vascular remodeling in the anatomic natural history of coronary atherosclerosis and in predicting clinical events. Briefly, the study involved 506 patients with acute coronary syndromes who underwent percutaneous coronary intervention (PCI) for the culprit lesion. The patients underwent 3-vessel VP at the time of the index catheterization procedure, under stable conditions after PCI of the culprit lesion and staged PCI of nonculprit lesions.
The present study included 496 patients who underwent VP at baseline and whose data were available. A total of 1,341 vessels obtained from these patients were analyzable (2.7 vessels/patient). Eighteen vessels exhibited very slow flow, rendering the flow measurement unreliable, and were excluded from the analysis for the indicated reasons: 5 vessels with flow-limiting stenoses, 13 vessels with Thrombolysis In Myocardial Infarction (TIMI) flow grade <3 despite revascularization of the culprit vessel in acute coronary syndromes, and 1 vessel that supplied collateral flow to a totally occluded vessel. A total of 1,322 vessels were eligible for this study.
Coronary artery dominance was classified into 3 types on the basis of angiography (right-dominant, left-dominant, and balanced circulation) according to whether the right coronary artery or the left circumflex coronary artery (LC), respectively, gave rise to the posterior descending artery. Balanced circulation was defined when the right coronary artery and LC supplied the posterior descending artery.
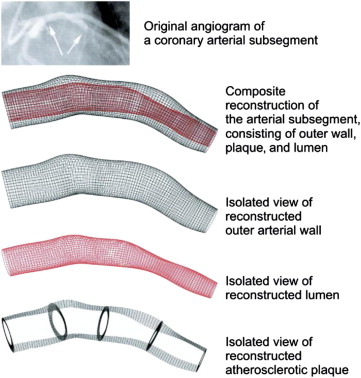
Our VP method for coronary blood flow measurement has been previously described. In brief, the 3-dimensional (3D) anatomy of the coronary artery was reconstructed from 2 planes of coronary angiography and electrocardiographically gated intravascular ultrasound (IVUS) images. The arterial lumen and outer vessel wall were reconstructed from digitized and segmented end-diastolic IVUS frames, using a semiautomated system to trace the lumen and external elastic membrane borders. The physical 3D path of the IVUS transducer during pullback was determined by using the corresponding angiographic projections. The 3D reconstructed catheter core served as the stem on which to rebuild the 3D geometry. The 3D position of each electrocardiographically gated IVUS frame was determined from the reconstructed trajectory of catheter pullback and pullback speed. The rotation of the frame was determined using computational geometry. Each frame was aligned perpendicular to the catheter core. The boundary points of each frame were connected by spline curves to rebuild the luminal geometry in 3D space ( Figure 1 ). Coronary blood flow for the arterial section being studied, a section chosen free of significant side branches that may significantly alter the flow, was calculated directly from the time required for the volume of blood contained within the section to be displaced by radiopaque material during a contrast injection. The true 3D volume of the segment was first calculated from the luminal borders, as described earlier. The number of cine frames required for the contrast media to pass from the inlet of the section to the outlet was counted. The coronary blood flow volume (milliliters per minute) was calculated as 30 frames/s × volume (ml)/frame count × 60.
Values are presented as mean ± SD for continuous variables and as numbers and percentages for categorical variables. Because the sample size of the patients with balanced circulation was too small to permit statistical comparison, the study population was divided into 2 groups (right-dominant and left-dominant or balanced circulation) in the comparative analysis. Differences between the 2 groups were assessed using Student’s t tests or Mann-Whitney U tests for continuous data and chi-square tests for categorical variables. All probability values are 2 sided, and p values <0.05 were considered statistically significant. Statistical analysis was performed using SPSS version 12.0 (SPSS, Inc., Chicago, Illinois).
Results
Patient and angiographic characteristics are listed in Table 1 . The numbers of patients with right-dominant, left-dominant, and balanced circulation were 453 (91.3%), 40 (8.1%), and 3 (0.6%), respectively. The number of right coronary arteries with VP data available was significantly smaller for left-dominant or balanced circulation than for right-dominant circulation because the right coronary artery in left-dominant circulation was generally too small to perform IVUS.
| Variable | Right-Dominant Circulation (n = 453) | Left-Dominant or Balanced Circulation (n = 43) | p Value |
|---|---|---|---|
| Age (yrs) | 65 ± 11 | 63 ± 12 | 0.521 |
| Men | 358 (79%) | 39 (91%) | 0.067 |
| Systolic blood pressure (mm Hg) | 128 ± 22 | 125 ± 17 | 0.375 |
| Diastolic blood pressure (mm Hg) | 73 ± 13 | 73 ± 12 | 0.729 |
| Heart rate (beats/min) | 70 ± 11 | 71 ± 10 | 0.578 |
| Hypertension ∗ | 288 (64%) | 25 (58%) | 0.48 |
| Dyslipidemia † | 385 (85%) | 40 (93%) | 0.151 |
| Diabetes mellitus | 153 (34%) | 22 (51%) | 0.023 |
| Previous myocardial infarction | 31 (7%) | 4 (9%) | 0.547 |
| Hematocrit (%) | 39 ± 5 | 40 ± 5 | 0.082 |
| Number of studied coronary arteries | |||
| LAD | 415 (92%) | 39 (91%) | 0.713 |
| LC | 403 (89%) | 41 (95%) | 0.410 |
| Right | 418 (92%) | 6 (14%) | <0.001 |
| 3-vessel available | 342 (76%) | 5 (12%) | <0.001 |
| Culprit vessel of acute coronary syndromes | |||
| LAD | 240 (53%) | 29 (67%) | 0.069 |
| LC | 67 (15%) | 14 (33%) | 0.003 |
| Right | 149 (33%) | 0 | <0.001 |
| Presence of ramus intermedius | 114 (25%) | 7 (16%) | 0.195 |
∗ Systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg or current use of antihypertensive medication.
† Low-density lipoprotein cholesterol ≥100 mg/dl and/or high-density lipoprotein cholesterol <40 mg/dl or current use of cholesterol-lowering medication.
The coronary blood flow of the LC was significantly higher in left-dominant or balanced circulation than in right-dominant circulation (113 ± 43 vs 72 ± 37 ml/min, p <0.001), whereas that of the right coronary artery was significantly lower in left-dominant or balanced circulation than in right-dominant circulation (56 ± 40 vs 113 ± 49 ml/min, p = 0.003). There was no significant difference in left anterior descending coronary artery (LAD) flow between the 2 groups (90 ± 37 vs 84 ± 40 ml/min, p = 0.273). There was also no significant difference in the total blood flow volume between the 2 groups ( Table 2 ).
| Coronary Blood Flow Volume (ml/min) | Right-Dominant Circulation (n = 453) | Left-Dominant or Balanced Circulation (n = 43) | p Value |
|---|---|---|---|
| LAD | 84 ± 40 (415) | 90 ± 37 (39) | 0.273 |
| LC | 72 ± 37 (403) | 113 ± 43 (41) | <0.001 |
| Right coronary artery | 113 ± 49 (418) | 56 ± 40 (6) | 0.003 |
| Total | 270 ± 82 (342) | 267 ± 49 (5) | 0.652 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


