Atherosclerotic lesions in the thoracic aorta detected by transesophageal echocardiography (TEE) have been correlated with coronary artery disease (CAD). We determined whether simple or complex aortic plaques seen on transesophageal echocardiogram correlated with extent, location, and severity of CAD. The study population consisted of 188 patients who underwent TEE and coronary angiography. Atherosclerotic plaques seen on transesophageal echocardiogram were defined as (1) complex plaques in the presence of protruding atheroma ≥4-mm thickness, mobile debris, or plaque ulceration or (2) simple plaques in the absence of findings consistent with complex plaques. Extent of CAD was grouped into 4 groups according to number of coronary vessels with ≥70% stenosis. Numbers of patients with CAD with 0-, 1-, 2-, and 3-vessel disease were 99, 31, 28, and 30 respectively. Compared to patients without CAD, patients with CAD (n = 89) had a significantly greater prevalence of aortic atherosclerotic plaques irrespective of degree of plaque complexity or location (p <0.05). Multivariate analysis found that hypertension (odds ratio 3.0, 95% confidence interval 1.3 to 7.0, p = 0.013), diabetes mellitus (odds ratio 2.4, 95% confidence interval 1.1 to 4.9, p = 0.022), and aortic plaque (odds ratio 3.8, 95% confidence interval 1.8 to 8.2, p = 0.001) were significantly associated with CAD. There was a significant relation between simple and complex aortic plaques with increasing severity of CAD (p <0.001). Multivariate logistic regression analysis showed that complex plaque in the descending aorta (odds ratio 5.4, 95% confidence interval 1.8 to 16.4, p = 0.003) was the strongest predictor of CAD. In conclusion, simple and complex thoracic atherosclerotic plaques detected by TEE are associated with increasing severity of CAD. Complex plaque in the descending aorta was the strongest association with presence of CAD.
Detection of atherosclerotic lesions in the aorta by transesophageal echocardiography (TEE) has been shown to be associated with coronary artery disease (CAD). Also, several autopsy studies have demonstrated a correlation between atherosclerosis scores in the thoracic aorta and in the coronary arteries. Conversely, absence of atherosclerotic lesions in the thoracic aorta has been reported to indicate absence of significant CAD. No studies have shown that transesophageal echocardiographic findings can replicate data reported at autopsy regarding the relation between aortic atherosclerosis and CAD. The purpose of the present study was to determine the correlation between the presence, location, and severity of atherosclerotic plaques in the thoracic aorta identified by TEE and presence and extent of coronary artery disease identified by coronary angiography.
Methods
In total 1,112 patients underwent TEE in the Pauley Heart Center at the Virginia Commonwealth University Hospitals (Richmond, Virginia) from August 2006 to July 2008. In a retrospective review of these patients, 201 patients underwent cardiac catheterization and coronary angiography for clinical indications within the 10 days preceding or the 10 days after TEE. Thirteen patients with previous coronary artery bypass surgery and/or previous percutaneous coronary intervention were excluded from the study population. In total 188 patients were included in the study. Indications for TEE were standard clinical indications and included evaluation of valvular heart disease, to rule out a cardiac source of embolism or thrombus, to determine presence of an intracardiac shunt, to evaluate for possible endocarditis, and as a screening procedure before intervention in the electrophysiologic laboratory. The study protocol was approved by the institutional review board of the Virginia Commonwealth University School of Medicine.
Coronary angiography was performed in the conventional manner with coronary stenosis assessed and quantified in multiple views. Significant disease was considered present if there was stenosis ≥70% in an epicardial vessel or 1 of its major branches. Indications for coronary angiography were standard clinical indications to identify presence, severity, and extent of coronary atherosclerosis.
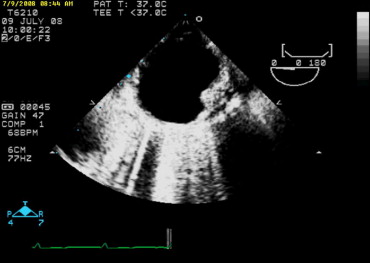
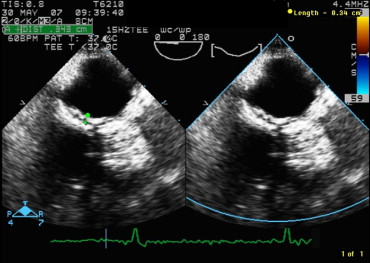
All patients underwent TEE using a multiplane probe with a Sonos 5500 system (Philips Medical Systems, Andover, Massachusetts). The ascending aorta, aortic arch, and proximal descending aorta were visualized in all patients. Atherosclerotic plaques were defined as presence of irregular and circumscribed intimal thickening with increased echogenicity of ≥1 segment of the thoracic aorta. Plaques were defined as complex if there was protruding atheromatous plaque ≥4-mm thickness, mobile debris, or plaque ulceration ( Figure 1 ). Plaques that were <4-mm thickness and lacked morphologic features of complex atherosclerosis were defined as simple plaques ( Figure 2 ). When multiple atheromatous plaques were present, the most advanced lesion was used to classify degree of atherosclerosis.
Clinical characteristics were expressed as mean ± SD or number (percentage). Assessment of the association of aortic atherosclerosis with CAD was performed in 2 steps. The first step was to compare the incidence of thoracic aortic atherosclerosis (of any degree and in any segment) to presence of CAD. The second step was to correlate simple and complex atheroscleroses in patients with extent of CAD. Logistical regression analysis was then used to assess whether aortic atherosclerosis of any degree and/or involving ≥1 aortic segment was associated with significant CAD. Variables included in the model were age, gender, race, and coronary risk factors (hypertension, diabetes, tobacco use) to determine to what degree and in which segment atherosclerosis had the greatest association with CAD. Pearson chi-square analysis was used to compare the discrete variables among groups. A p value <0.05 was considered statistically significant. SPSS 14.0 (SPSS, Inc., Chicago, Illinois) was used for all analyses.
Results
Clinical characteristics of the 188 patients (111 men and 77 women, mean age 57 ± 13 years) are listed in Table 1 . Significant disease of ≥1 coronary artery (CAD) was present in 89 patients (47%); 99 patients (53%) had normal coronary arteries or nonsignificant luminal disease. There was a significantly higher incidence of cardiovascular risk factors, including hypertension, diabetes mellitus, hypercholesterolemia, and cigarette smoking, in patients with CAD.
| Variable | CAD | p Value | |
|---|---|---|---|
| No (n = 99) | Yes (n = 89) | ||
| Age (years) | 57 ± 13 | 62 ± 11 | 0.12 |
| Men | 56 (57%) | 55 (62%) | 0.47 |
| Women | 43 (43%) | 34 (38%) | 0.47 |
| Black | 58 (59%) | 42 (47%) | 0.14 |
| Caucasian | 37 (37%) | 44 (49%) | 0.095 |
| Other race | 4 (4%) | 2 (2%) | 0.49 |
| Hypertension | 64 (65%) | 76 (85%) | 0.001 |
| Diabetes mellitus | 24 (24%) | 44 (49%) | <0.001 |
| Hypercholesterolemia ⁎ | 11 (11%) | 13 (14%) | 0.47 |
| Smoker | 33 (33%) | 41 (46%) | 0.074 |
Patients with significant CAD (n = 89) had a significantly higher incidence of atherosclerotic plaques. Simple and complex atherosclerotic plaques were seen with significantly greater frequency in the ascending aorta, aortic arch, and descending aorta in these patients compared to patients with normal coronary arteries (n = 99, p <0.05; Table 2 ). Numbers of patients with significant 1-, 2-, and 3-vessel CAD are presented in Table 3 . There was a significant relation between simple plaque and complex plaques in any segment of the thoracic aorta and severity and extent of CAD (p <0.001).
| Variable | CAD | p Value | |
|---|---|---|---|
| No (n = 99) | Yes (n = 89) | ||
| Aortic plaque (of any degree and any aortic segments) | 39 (39%) | 71 (80%) | <0.001 |
| Simple plaque (of any aortic segment) | 25 (25%) | 46 (52%) | <0.001 |
| Complex plaque (of any aortic segment) | 12 (12%) | 37 (42%) | <0.032 |
| Ascending aortic plaque (of any degree) | 3 (3%) | 10 (11%) | 0.025 |
| Aortic arch plaque (of any degree) | 28 (28%) | 44 (49%) | 0.002 |
| Descending aortic plaque (of any degree) | 33 (33%) | 66 (74%) | <0.001 |



