Reflex Sympathetic Dystrophy: A Type I Complex Regional Pain Syndrome
Reflex Sympathetic Dystrophy: A Type I Complex Regional Pain Syndrome
Dennis F. Bandyk
Since the time of the American Civil War, the clinical diagnosis and management of chronic pain syndromes following extremity nerve, bone, and associated soft tissue trauma have been characterized further. The nomenclature used to describe these syndromes varies with clinical site, etiology, symptoms, and physical signs. The entity of burning pain, sympathetic hyperactivity, hyperesthesia, joint stiffness, muscle atrophy, and skin changes following extremity injury has been described by a multiplicity of terms, including reflex sympathetic dystrophy, causalgia, mimocausalgia, shoulder-hand syndrome, Sudeck atrophy, posttraumatic dystrophy, and reflex neurovascular dystrophy. Knowledge of chronic pain syndromes is relevant to vascular surgeons, because many patients are initially referred for evaluation of extremity pain, cyanosis, skin temperature changes, and edema—all of which can imitate arterial or venous disease.
In 1995, the International Association for the Study of Pain proposed using the term complex regional pain syndromes (CRPS) to describe chronic pain syndromes and defined two Types (I and II) to portray specific clinical features. Type I CRPS was recommend to replace the term reflex sympathetic dystrophy (RSD), while Type II included equivalent clinical symptoms of RSD, but a peripheral nerve injury is documented as the initiating factor for the CRPS. The symptoms of causalgia accompanying a peripheral nerve injury are therefore a Type II CRPS. Because the CRPS classification is not widely used by practitioners, the diagnosis of RSD remains rooted in the diagnostic terminology in communications with patients, physicians, third-party payers, and for determinations of medical disability.
Reflex Sympathetic Dystrophy (Type I CRPS)
The symptoms and signs of burning extremity pain, sympathetic hyperactivity, muscle wasting, joint stiffness, and trophic skin changes characterize RSD, a poorly understood and frequently underdiagnosed condition following trauma. It is estimated that the prevalence of CRPS following peripheral nerve injury is 2% to 5%, 1% to 2% after bone fracture, and <1% after soft tissue contusion or surgical procedures. The pathophysiology of RSD is related to sympathetic nerve dysfunction and involves three nervous system mechanisms:
Increased afferent impulses from peripheral nerves after injury due to irritation or increased sensitivity to norepinephrine released by sympathetic postganglion neurons
Regenerating primary afferents from artificial synapses with regenerating sympathetic neurons
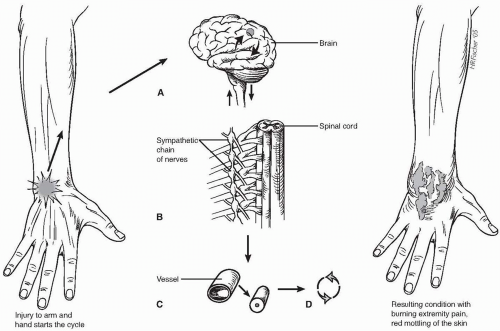
Increased stimulation in the internuncial pool located in the anterior horn of the spinal cord with “opening the gate” and transmission of increased impulses to the brain for perception of pain (Fig. 64-1).
Hypothetically, the chronic disturbance in sympathetic nervous system function triggers an inflammatory response leading to cyclical vasospasm, which results in mottled skin, swelling, and burning extremity pain. The RSD condition has been described in both children and adults, typically developing in young active adults (age 20 to 30 years), and there appears to be no gender predisposition. Its development has been associated with a variety of conditions (Table 64-1), with the common denominator being injury to the extremity. The best way to describe RSD is in terms of an extremity injury caused by trauma, infection, surgery, or a repetitive motion disorder, i.e., carpal tunnel syndrome that does not follow the normal healing path. Development does not appear to depend on the magnitude of injury, and diagnosis may be hampered by a lack of objective findings or by legal issues, i.e., accusation of malingering to obtain medical disability.
In 1959, Drucker et al. described three clinical stages of RSD, with progression of symptoms and disability occurring in an unpredictable manner with time (Table 64-2). In Stage I RSD, extremity pain is localized to the region or site of injury, and its severity has increased during the healing process. Tenderness in the affected extremity is typically out of proportion to what is expected on physical examination, and the pain is described as constant with features of burning or a deep ache. Allodynia (pain with repetitive soft contact) may be present, and the escalation in tenderness at the site of repetitive tactile stimulation may persist for an extended period of time (hyperpathia). Trigger points as seen with other myofascial pain syndromes may be present on physical examination. Progression of symptoms characterizes Stage II RSD, with development of visible skin changes, including dryness, cyanosis or rash, muscle atrophy, and joint immobility. Cold sensitivity is present in all RSD stages and may be associated with other manifestations of excessive sympathetic tone, including hyperhidrosis and pilomotor changes. Abnormalities of either hair and nail growth or texture can occur in Stage II RSD. Limb swelling is a common sign of RSD progression and may develop into a hard, brawny form of lymphedema localized to the most painful portion of the extremity. Muscle and joint stiffness associated with decreased extremity range of motion, involuntary spasms, and limb disuse are signs of advanced RSD.
Figure 64-1. Involvement of the sympathetic nervous system in the reflex sympathetic dystrophy following extremity trauma. Injury to the arm and hand begins the cycle. A: The original injury initiates a pain impulse carried by sensory nerves to the central nervous system. B: The pain impulse in turn triggers an impulse in the sympathetic nervous system that returns to the original site of injury. C: The sympathetic impulse triggers the inflammatory response, which causes the vessels to spasm and leads to swelling and increased pain. D: The pain triggers another response, establishing a cycle of pain and swelling. This results in burning, extremity pain, and red mottling of the skin.
Table 64-1 Conditions Associated with Development of Reflex Sympathetic Dystrophy (RSD)
Trauma, including musculoskeletal sprain or contusion
Repetitive motion disorder
Soft tissue infection
Carpal/tarsal tunnel syndrome
Osteoarthritis
Cervical and lumbar disk disease
Surgery
Thrombophlebitis
Venapuncture
Table 64-2 Classification of Reflex Sympathetic Dystrophy Severity+
Stage I
Onset of severe pain limited to the site of injury
Skin sensitivity to touch and light pressure (hyperesthesia)
Localized swelling
Muscle cramps
Stiffness and limited mobility
Skin color/temperature changes from erythema/warm to cyanosis/cold
Increased sweating (hyperhidrosis)
Stage II
Diffuse severe pain not limited to site of injury
Spreading limb swelling that may change from soft to brawny
Changes in hair (coarse, scant) and nails (growth changes, brittle, grooved)
Spotty wasting of bone begins (osteoporosis)
Muscle atrophy
Stage III
A. Marked irreversible muscle atrophy occurs
B. Intractable pain
C. RSD may spread to other regions of the body
+Adopted from Druker et al. Pathogenesis of posttraumatic sympathetic dystrophy. Am J Surg. 1959;87:454-465 and Clinical Practice Guidelines of Reflex Sympathetic Dystrophy Syndrome of America (www.rsds.org).
In Stage III RSD, symptoms of pain can spread to involve the trunk, face, and other extremities, and this is termed spreading RSD. The pain of the originally involved limb is often intractable, and irreversible muscle atrophy can develop. When symptoms develop at only a remote site without an identifiable traumatic event, it is termed “independent type” of RSD and may be associated with signs of excessive sympathetic activity. As RSD symptoms/signs progress, the likelihood that symptoms are relieved by sympathetic nerve blocks decreases, i.e., a sympathetic-independent RSD condition develops.
The onset of RSD symptoms following extremity trauma is variable and typically develops within weeks of the injurious event. RSD pain and disability are often characterized by intervals of exacerbation and partial remission. With medical and rehabilitation treatment, including using sympathetic nerve block therapy, spontaneous resolution of RSD symptoms can occur; however, the extremity remains at risk for recurrence months to years later. In the majority of patients, the RSD syndrome evolves into a chronic, permanent disability affecting daily activities, ability to work, and social relationships.
Diagnosis
The clinical hallmark of RSD is extremity pain and mobility problems out of proportion to that expected from the original injury. The diagnosis of RSD may be delayed due to its varied clinical presentation and lack of a definitive test. The treating physician may be uninformed regarding the clinical features of RSD and attribute failure to heal to erroneous mechanisms or malingering. Often a delay in diagnosis occurs because of partial remission that the patient and physician may perceive do the result of prescribed therapy or the “tincture of time.” It requires an astute clinician to appreciate the cyclic nature of the RSD condition, carefully review the often-complex medical history, and consider referral to a multidisciplinary pain clinic. An extended evaluation period is typical while the patient’s pain pattern and associated extremity disability progresses. A multidisciplinary approach to the CRPS patient is recommended to exclude other musculoskeletal or peripheral nerve conditions that may contribute to extremity pain, swelling, and disability.
The nature and severity of extremity pain should be determined. A visual analogue pain severity scale is useful to document pain severity at each evaluation. The patient grades the basal pain severity on a scale of 0 to 10, where 0 is no pain, 5 is pain that interferes with daily/work activities, and 10 is the worst pain imaginable. The typical RSD patient rates the pain severity in the 7 to 8 ranges with exacerbations to 10 occurring daily. This level of pain interferes with all social activities, and the patient is commonly housebound.
The site of injury should be evaluated for residual soft tissue, musculoskeletal, and nerve injury. Invariably, the vascular examination is normal and should include documentation of normal limb and digits systolic blood pressure. The deep and superficial extremity veins should be assessed by duplex ultrasound for patency and normal vein valve function. A careful examination of the musculoskeletal system is mandatory, including joint space effusion, limb range-of-motion, and assessment of muscle. Careful assessment for muscle atrophy should be performed, with measurement of limb girth and comparison with unaffected extremities. Documentation of skin color, moisture, and temperature assessment are necessary, and the patient should be questioned regarding excessive sympathetic tone under stressful conditions. The neurologic exam should focus on both motor and sensory function, and any nerve deficit should be recorded.
Only gold members can continue reading. Log In or Register to continue