This study sought to quantitatively evaluate the reduction of radiation dose in coronary angiography and angioplasty with the use of image noise reduction technology in a routine clinical setting. Radiation dose data from consecutive 605 coronary procedures (397 consecutive coronary angiograms and 208 consecutive coronary interventions) performed from October 2014 to April 2015 on a coronary angiography system with noise reduction technology (Allura Clarity IQ) were collected. For comparison, radiation dose data from consecutive 695 coronary procedures (435 coronary angiograms and 260 coronary interventions) performed on a conventional coronary angiography system from October 2013 to April 2014 were evaluated. Patient radiation dosage was evaluated based on the cumulative dose area product. Operators and operator practice did not change between the 2 evaluated periods. Patient characteristics were collected to evaluate similarity of patient groups. Image quality was evaluated on a 5-grade scale in 30 patients of each group. There were no significant differences between the 2 evaluated groups in gender, age, weight, and fluoroscopy time (6.8 ± 6.1 vs 6.9 ± 6.3 minutes, not significant). The dose area product was reduced from 3195 ± 2359 to 983 ± 972 cGycm 2 (65%, p <0.001) in coronary angiograms and from 7123 ± 4551 to 2431 ± 1788 cGycm 2 (69%, p <0.001) in coronary interventions using the new noise reduction technology. Image quality was graded as similar between the evaluated systems (4.0 ± 0.7 vs 4.2 ± 0.6, not significant). In conclusion, a new x-ray technology with image noise reduction algorithm provides a substantial reduction in radiation exposure without the need to prolong the procedure or fluoroscopy time.
This study aims to quantify the radiation dose reduction in coronary angiography and coronary angioplasty in a routine clinical setting by the use of the new imaging system.
Methods
Consecutive patients undergoing coronary angiography and angioplasty in a catheterization laboratory exclusively used for coronary angiography and coronary angioplasty at the Bonifatius Hospital Lingen (Lingen, Germany) were included in this study. Patients were included from 2 periods (period A: January 2014 to June 2014 and period B: November 2014 to April 2015). During period A, patients were studied on a conventional biplane angiography system. After replacement of the system, patients were studied during period B on a biplane angiography system with an image processing chain for noise reduction in fluoroscopy. A total of 1,295 patients were included in the study, 690 patients during period A and 605 patients during period B. Patient characteristics and procedural characteristics are given in Table 1 . No patient was excluded for poor renal function or high body mass index (BMI). There were no changes in operators or operator techniques between the 2 study periods. In 84% the access site has been the radial artery for invasive and interventional procedures during period A and in 85% in period B. To evaluate the impact of BMI on the reduction of radiation dosage, 3 different BMI groups were evaluated; group A: BMI below 20 kg/m 2 , group B: BMI 20 to 30 kg/m 2 , and group C: BMI above 30 kg/m 2 . Procedures were divided into diagnostic and interventional. Procedures with ad hoc intervention were counted as interventional only. Procedural data such as fluoroscopy time and contrast medium volume were collected to compare procedure complexity. The cumulative dose area product in cGycm 2 was determined as indicator of radiation dose.
| Coronary angiography | Reference Patients | Noise reduction Patients |
|---|---|---|
| (N=431) | (N=397) | |
| Age (years) | 66.5±12.1 | 67.7±12.2 |
| Men | 276 (64%) | 255 (64%) |
| Weight (kg) | 84.0±18.4 | 86.2±20.0 |
| Size (cm) | 172.1±9.4 | 171.9±9.8 |
| Body mass index (kg/m 2 ) | 28.3±5.3 | 28.8±5.0 |
| Coronary angioplasty | (N=259) | (N=208) |
| Age (years) | 70.4±10.9 | 69.0±11.6 |
| Men | 173 (67%) | 139 (67%) |
| Weight (kg) | 84.8±16.3 | 87.0±18.8 |
| Size (cm) | 172.1±8.9 | 172.5±9.6 |
| Body mass index (kg/m 2 ) | 28.6±5.2 | 29.4±6.7 |
| All procedures | (N=690) | (N=605) |
| Age (years) | 68.0±11.8 | 68.1±11.8 |
| Men | 449 (65%) | 394 (65%) |
| Weight (kg) | 84.3±17.8 | 86.1±19.0 |
| Size (cm) | 172.1±11.1 | 172.1±14.5 |
| Body mass index (kg/m 2 ) | 28.4±5.4 | 29.0±5.6 |
During period A, a conventional biplane angiography system (Siemens BICOR HI-P/Hicor TOP; Siemens, Erlangen, Germany) was used. During period B, a biplane flat panel angiography system with advanced real-time image noise reduction algorithms and optimized acquisition chain for fluoroscopy and exposure techniques (Allura Xper FD 20/10; Philips Healthcare, Best, the Netherlands, with Clarity IQ technology) was used. The real-time image noise reduction algorithm (Clarity IQ) uses several features to allow reduction of radiation dose. Noise reduction consists of both temporal and spatial noise reduction. Temporal noise reduction refers to processing that is carried out over time, thus, over subsequent images, and spatial noise reduction refers to processing carried out over an area within one image. Temporal noise is reduced by averaging several frames. The Clarity IQ noise reduction algorithm uses motion compensation by aligning moving structures before averaging. Thus, considering motion compensation, more frames can be used and stronger temporal filtering can be applied. The result is a better noise reduction for moving structures. Spatial noise reduction refers to finding the noise within a single image and filtering it out pixel by pixel. Pixels of the so-called neighborhood are considered for the spatial filtering algorithms. By averaging the pixel intensity of the surrounding, noise can be filtered out. By averaging larger neighborhoods due to more computational power, more noise can be reduced. Subsequently, by improved temporal and spatial noise reduction, more noise is reduced allowing less radiation dosage for similar image quality. Furthermore, the x-ray acquisition chain was optimized to allow patient radiation dose reduction with similar image quality.
For analysis of image quality, 30 randomly selected coronary angiograms were evaluated from each group. In each study, a cine run of the left coronary artery was evaluated. The projection had to be left anterior oblique 45° with a cranial angle of 20°. Image quality was assessed on a scale from 1 to 5 with 1 indicating poor image quality and 5 indicating excellent image quality. Reading of images was performed by 2 doctors blinded to the acquisition fashion. The assessment of the 2 doctors was averaged for each case.
Statistical analysis was performed using SPSS software, version 17.0 (SPSS, Inc., Chicago, Illinois). Categorical data are presented as frequencies and were compared using the Fischer’s exact test. Continuous data were presented as mean ± SD and compared using the Student t test or analysis of variance as adequate. Dose area product was related to BMI using linear regression analysis. A p <0.05 was considered significant.
Results
The fluoroscopy times between the 2 patient groups were similar. This finding relates to coronary angiography and coronary angioplasty procedures ( Table 2 ).
| Coronary angiography | Reference Patients | Noise reduction Patients | P |
|---|---|---|---|
| (N=431) | (N=397) | ||
| Fluoroscopy time (min) | 4.6±4.3 | 4.7±4.4 | n.s. |
| Contrast volume (cc) | 72.6±43.8 | 81.0±47.7 | n.s. |
| Dose area product (cGycm 2 ) | 3193±2358 | 984±975 | <0.001 |
| Coronary angioplasty | (N=259) | (N=208) | |
| Fluoroscopy time (min) | 10.4±6.9 | 11.1±7.1 | n.s. |
| Contrast volume (cc) | 170.2±69.1 | 175.2±73.1 | n.s. |
| Dose area product (cGycm 2 ) | 7123±4551 | 2430±1981 | <0.001 |
| All procedures | (N=690) | (N=605) | |
| Fluoroscopy time (min) | 6.8±6.1 | 6.9±6.3 | n.s. |
| Contrast volume (cc) | 109.1±72.3 | 113.4±73.5 | n.s. |
| Dose area product (cGycm 2 ) | 4663±3852 | 1478±1559 | <0.001 |
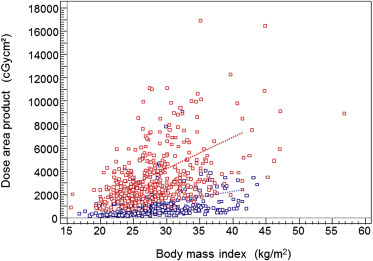
There was a substantial decrease of more than 60% in radiation dosage for both coronary angiography and coronary angioplasty procedures ( Table 2 ). Considering all procedures, the mean dose area product decreased from 4663 ± 3852 to 1477 ± 1556 cGycm 2 (p <0.001). Mean dose area product using the conventional system and considering all procedures was 3275 ± 3063 cGycm 2 for female patients and 5417 ± 4027 cGycm 2 for male patients. Considering the radiation noise reduction system, the mean dose area product was 1045 ± 1112 cGycm 2 for female patients and 1711 ± 1712 cGycm 2 for male patients. Mean dose area product with the conventional fluoroscopy system was 1672 ± 981 cGycm 2 in patients with a BMI <20 kg/m 2 , 4094 ± 3482 cGycm 2 in patients with a BMI 20 to 30 kg/m 2 and 6009 ± 4249 cGycm 2 in patients with a BMI ≥30 kg/m 2 . Considering the radiation noise reduction system, mean dose area product was 556 ± 369 cGycm 2 in patients with a BMI <20 kg/m 2 , 1261 ± 1175 cGycm 2 in patients with a BMI 20 to 30 kg/m 2 and 1899 ± 2015 cGycm 2 in patients with a BMI ≥30 kg/m 2 . Thus, the mean reduction in dose area product was equal between the 3 BMI groups (67%, 69%, and 68%, respectively). There was a correlation of patient dose area product with the BMI considering conventional and image noise reduction technology. However, considering the image noise reduction technology, the regression line was on a significantly lower dose area product level ( Figure 1 ).