Figure 17.1
Standard posterolateral thoracotomy incision. LD latissimus dorsi muscle
Right Upper Lobectomy
The lung is retracted laterally to place the superior hilar vessels on tension. The mediastinal pleura over the superior pulmonary vein is incised to delineate the entire extent of the upper lobe vein. The superior extent is where the vein meets the truncus arteriosus, whereas the inferior extent is at the takeoff of the middle lobe vein. Care must taken to identify the middle lobe vein inferiorly and to preserve it. There often are hilar lymph nodes in these two areas, and they should be excised or mobilized away from the vein if possible. Before isolation and division of the upper lobe vein, the ongoing pulmonary artery should be identified and avoided. Once isolated, the upper lobe vein may be ligated and divided either with ties and scissors or by endovascular stapling. Next, the truncus arteriosus is mobilized from the surrounding hilar lymph nodes inferiorly and the upper lobe bronchus posteriorly and divided (Fig. 17.2). At this juncture, if the hilar and peribronchial lymph nodes have not been excised previously, they should be removed completely. The lung is retracted anteriorly, and the posterior pleura between the bronchus intermedius and the upper lobe bronchus is incised. The interlobar lymph nodes are removed, exposing the posterior ascending branch of the upper lobe and the upper lobe bronchus (Fig. 17.3). These two remaining hilar structures may then be divided in whatever order is most practical and easiest. The bronchus typically is stapled with a 4.8-mm stapler or may be divided sharply and sewn closed with 3-0 or 4-0 absorbable sutures. Lastly, the horizontal fissure is completed with multiple firings of a linear stapler.
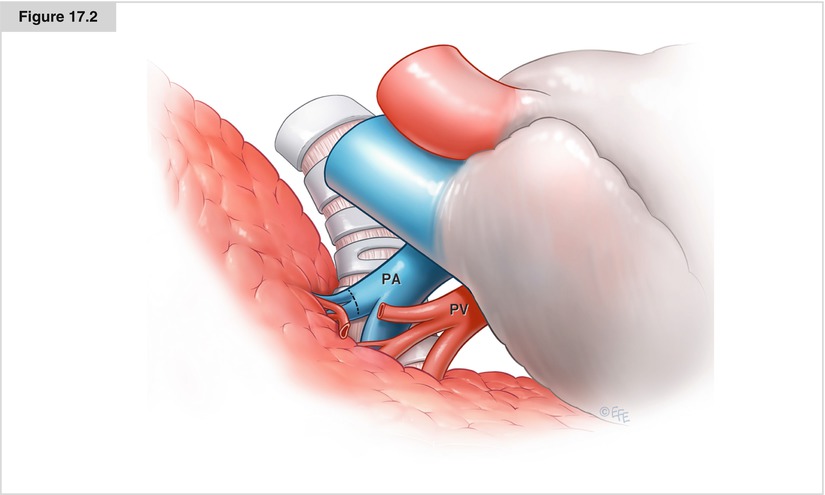
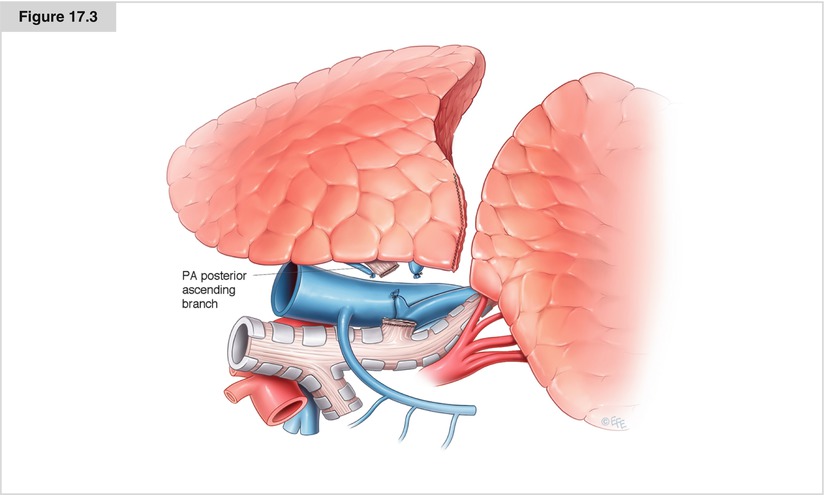
Figure 17.2
Isolation and division of the truncus arteriosus following division of the right upper lobe superior vein. PA pulmonary artery, PV pulmonary vein
Figure 17.3
Exposure of the posterior ascending branch of the pulmonary artery following division of the right upper lobe bronchus. PA pulmonary artery
Middle Lobectomy
The right lower and middle lobes are allowed to separate naturally, and the major fissure is explored. The mediastinal pleura overlying the anterior portion of the fissure between the middle and lower lobes is divided by cautery or sharply. Identification and excision of the interlobar lymph nodes will expose the basilar pulmonary artery and the takeoff of the middle lobe bronchus. The lung is retracted laterally, and the mediastinal pleura between the lower lobe and middle lobe pulmonary veins is divided. If the fissure is complete, the remaining anterior pleura may be divided with cautery. If it is incomplete, a stapler may be used to complete the fissure anteriorly. The middle lobe vein is isolated and divided (Fig. 17.4). The hilar and peribronchial lymph nodes are excised to expose the middle lobe bronchus, which is then isolated and divided (Fig. 17.4 inset). The remaining middle lobe artery or arteries are easily identified, isolated, and divided. The lobectomy is then completed by division of the horizontal fissure.

Figure 17.4
Exposure of the middle lobe bronchus following division of the middle lobe vein. Inset shows exposure of the middle lobe pulmonary artery branches. PA pulmonary artery, PV pulmonary vein
Right Lower Lobectomy
The inferior pulmonary ligament is divided by cautery up to the inferior pulmonary vein. The inferior ligament lymph nodes are excised, and the pleura is divided posteriorly up to the level of the takeoff of the right upper lobe bronchus and anteriorly up to the level of the middle lobe vein. The hilar nodes between the upper lobe and bronchus intermedius and between the middle and lower lobe veins are excised. The inferior pulmonary vein is isolated. The right lower and middle lobes are allowed to separate naturally, and the major fissure is explored. The mediastinal pleura overlying the anterior portion of the fissure is divided sharply or by cautery. As in the middle lobectomy, identification and excision of the interlobar lymph nodes will expose the basilar pulmonary artery and the takeoff of the middle lobe bronchus. If the fissure is complete, the remaining pleura of the anterior portion of the major fissure may be divided with cautery. If it is incomplete, a stapler may be used to divide it. The inferior vein is divided (see Fig. 17.5), and the lung is retracted cephalad. The plane between the lower lobe bronchus and basilar artery is developed, and the bronchus is isolated and stapled (Fig. 17.5 inset). Once the vein and bronchus are divided, the only remaining structures are the basilar pulmonary artery and the posterior aspect of the major fissure (Fig. 17.5 inset). Lastly, the basilar pulmonary artery is isolated and divided, and the remaining posterior portion of the major fissure is completed.
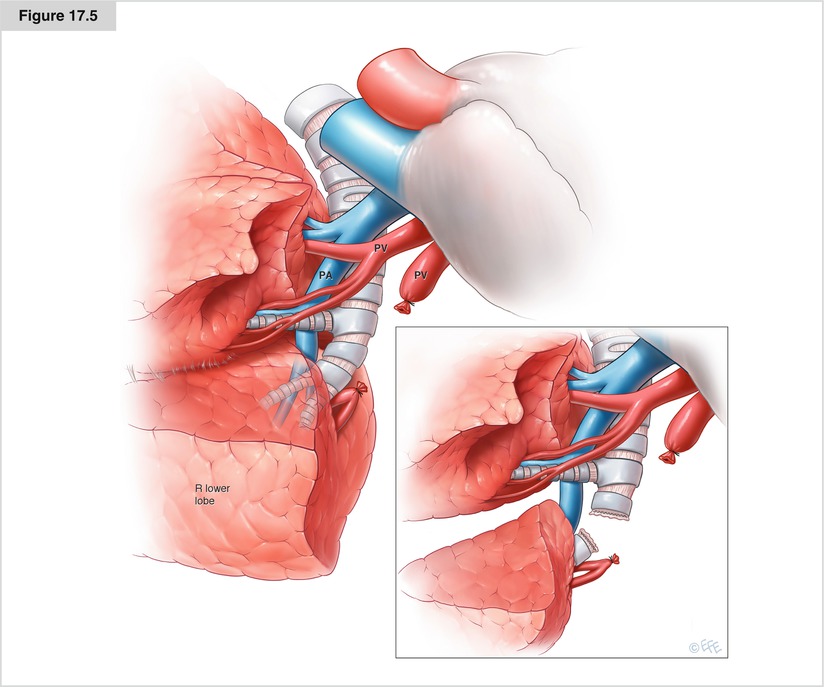
Figure 17.5
Isolation and division of the inferior pulmonary vein. Inset shows division of the right lower lobe bronchus revealing the remaining basilar pulmonary artery. PA pulmonary artery, PV pulmonary vein
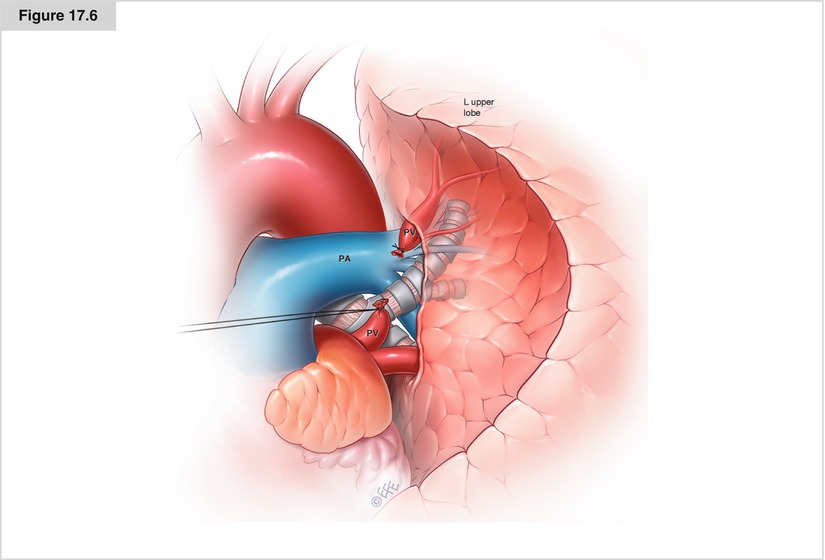
Left Upper Lobectomy
The lung is retracted laterally to place the superior hilar vessels on tension. The mediastinal pleura over the superior pulmonary vein is incised to delineate the entire extent of the upper lobe vein. The superior extent is where the vein meets the left main pulmonary artery, whereas the inferior extent is at the junction of the superior and inferior veins. The superior vein is divided (Fig. 17.6), and the mediastinal pleura is further divided superiorly and posteriorly around the entire superior hilum. The hilar lymph nodes between the upper lobe bronchus and the apicoposterior pulmonary artery branch are excised or mobilized. The apicoposterior branch is isolated and ligated (Fig. 17.7). The peribronchial and interlobar lymph nodes between the upper and lower lobe bronchi are removed. The upper lobe bronchus is then exposed (Fig. 17.7) and divided. The lung is retracted posteriorly to expose the remaining pulmonary artery branches, including the anterior, lingular, and any additional posterior branches. These are sequentially isolated and divided (Fig. 17.7). Alternatively, the left upper lobe arterial branches may be isolated and divided posteriorly before division of the bronchus if the need arises or based on surgeon preference (Fig. 17.8). Once the remaining arterial branches have been ligated, the major fissure is completed with multiple firings of the stapler.