Pulmonary Embolism and Deep Venous Thrombosis
GENERAL PRINCIPLES
• Acute pulmonary embolism (PE) is a commonly diagnosed condition with a morbidity and mortality rate that varies by age, clinical presentation, and the presence of comorbid disease.
• Despite advances in diagnosis and management, PE remains an underdiagnosed condition.
• Untreated PE has a high mortality rate. In some cases, PE can be safely treated at home, while in others immediate admission to an intensive care unit may be required to prevent death.
• Accurate risk stratification remains a critical component of the initial evaluation of the patient with acute PE.
• Effective approaches for the evaluation of patients with suspected PE and the treatment of those diagnosed with PE exist.
Definition
• Thromboses or blood clots occur in veins, arteries, or chambers of the heart.
• Venous thromboembolism (VTE) refers to the presence of deep vein thrombosis (DVT) or PE.
• Thrombus, air, fat, tumor, and foreign bodies may embolize to the lung.
• PE consists of embolized thrombus in the pulmonary arterial system.
Classification
• PE classification schema uses the terms acute versus chronic.
• Acute PE classification may use terms massive, submassive, and other.
• Massive PE, associated with acute right heart failure, leads to hypotension (e.g., systolic blood pressure <90 mm Hg or a drop >40 mm Hg from baseline for at least 15 minutes) despite volume resuscitation and vasopressor therapy. Hypotension may also occur from arrhythmias and decreased cardiac output.
• Submassive PE encompasses patients with PE who have hemodynamic stability in the setting of right ventricular (RV) dysfunction.
Epidemiology
• The overall annual incidence of PE has been reported ∼23–69 cases per 100,000. VTE incidence increases sharply after about 50 years of age and is consistently higher in males. Rates are also higher in Caucasians and African Americans than Hispanics and Asian-Pacific Islanders.1–3
• The introduction of contrast-enhanced multidetector helical chest CT scan (PE protocol CT) has been associated with a doubling of the incidence of PE.4,5
• Without treatment, half of patients with proximal lower extremity DVT develop PE.
• Autopsy studies suggest that many PEs remain undiagnosed.2
Etiology
• DVTs in the proximal lower extremities and pelvis produce most PEs.
• Only about one-half to three-quarters of the patients diagnosed with PE will have DVT found on venous compression ultrasound of the lower extremities.
• DVTs that occur in upper extremities, often secondary to an indwelling catheter, may also cause PE.
Pathophysiology
• Vascular obstruction may lead to increased pulmonary vascular resistance, which if severe enough can lead to acute right heart failure and shock.
 This occurs commonly in cases with emboli at main pulmonary arteries or bifurcations.
This occurs commonly in cases with emboli at main pulmonary arteries or bifurcations.
 The amount of clot burden also plays a role in the severity of hemodynamic compromise.
The amount of clot burden also plays a role in the severity of hemodynamic compromise.
• Inflammatory mediators also play a role in vasoconstriction of the pulmonary vasculature, decreased perfusion, and increased vascular resistance.
• Pulmonary arterial obstruction may produce hypoxemia via impaired alveolar gas exchange and increased lung dead space ventilation.
Risk Factors
• A method of classifying VTE risk factors uses the categories of inherited, acquired, or unknown (idiopathic).
• The most common inherited risk factors for VTE include two gene polymorphisms (factor V Leiden and prothrombin gene G20210A), deficiencies of the natural anticoagulants protein C, protein S, and antithrombin, dysfibrinogenemia, and hyperhomocysteinemia.
• Spontaneous (idiopathic) thrombosis, despite the absence of an inherited thrombophilia and detectable autoantibodies, predisposes patients to future thromboses.
• Acquired hypercoagulable states may arise secondary to malignancy, immobilization, infection, trauma, surgery, collagen vascular diseases, nephrotic syndrome, heparin-induced thrombocytopenia (HIT), disseminated intravascular coagulation (DIC), medications (e.g., estrogen), and pregnancy.
DIAGNOSIS
Clinical Presentation
• PE may produce shortness of breath, chest pain (pleuritic), hypoxemia, hemoptysis, pleural rub, new right-sided heart failure, and tachycardia, but these signs and symptoms are neither sensitive nor specific.
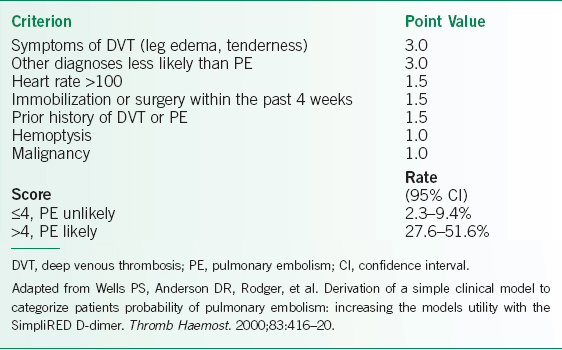
• Validated clinical risk factors for a PE in outpatients who present to an emergency department include signs and symptoms of DVT, high suspicion of PE by the clinician, tachycardia, immobility in the past 4 weeks, history of VTE, malignancy, and hemoptysis (see Table 21-1).6
• Clinical suspicion of DVT or PE should lead to objective testing.
• Patient symptoms are usually broad, nonspecific, and not sensitive.
• Dyspnea commonly occurs with PE. Other symptoms include pleuritic chest pain, cough, hemoptysis, lightheadedness, syncope, and diaphoresis.
• Vital signs are the most important physical examination findings in PE. Patients with PE often have tachycardia or tachypnea. Hypotension suggests possible massive PE and prompt diagnostic workup is essential.
• Other physical examination findings are very nonspecific, including rales, prominent S2 and P2 on cardiac auscultation, and elevated jugular venous pressure.
TABLE 21-1 MODIFIED WELLS CRITERIA FOR PULMONARY EMBOLISM
Differential Diagnosis
• Clinicians under diagnose PE because it mimics many other diseases and vice versa.
• The differential is broad and includes pneumonia, acute coronary syndrome, acute lung injury, pleuritis, pericarditis, and congestive heart failure.
• In a hypotensive patient, the differential broadens to include sepsis, hypovolemia, cardiac tamponade, and acute myocardial infarction.
Diagnostic Testing
• Pretest probability plays a key role in the workup of patients with suspected PE.
• The incorporation of pretest probability, using scores such as Wells score or Geneva score, with diagnostic tests improves the accuracy of diagnosis (Table 21-1).6–9
• CXR, ECG, and arterial blood gas all provide nonspecific information but they can assist in determining pretest probability and clinical severity, and evaluating for other disorders.
Laboratories
• d-Dimer and cross-linked fibrin degradation products may increase during PE but they are nonspecific and have a low positive predictive value (PPV) and specificity; patients with a positive test require further evaluation.
• A negative d-dimer in combination with low pretest probability can exclude almost all PEs.10
• In the setting of a moderate to high clinical pretest probability (e.g., patients with cancer), a negative d-dimer does not have sufficient negative predictive value (NPV) for excluding the presence of PE.
• Arterial blood gas may or may not show hypoxemia or an increased alveolar–arterial oxygen gradient.
• Cardiac biomarkers such as troponin and brain natriuretic peptide (BNP) are useful for assisting with prognosis but they have low diagnostic accuracy.11,12
Electrocardiography
• Sinus tachycardia occurs in most patients with PE.
• The classic findings on ECG of S1Q3T3 (S in V1, Q wave in V3, and T-wave inversion in V3) and right bundle branch block are uncommon and not diagnostic.
• Signs of RV strain that include right axis deviation and RV hypertrophy may suggest the presence of massive PE.
Imaging
• CXR usually shows no specific findings, but may help assess for other diagnoses in the most timely manner. Classic findings such as Westermark Sign and Hampton Hump rarely occur.
• The most common and important diagnostic modalities for assessing patients with suspected PE include multidetector helical chest CT and ventilation/perfusion scintigraphy (V/Q scan).
• The stability of the patient plays an important role in which diagnostic test to perform (see Fig. 21-1).13
• Contrast-enhanced multidetector helical chest CT scan (PE protocol CT) has become the gold standard test for evaluating patients for PE, and it may assist with the detection of alternative or concomitant diagnoses.14
 The sensitivity of CT for VTE improves by combining the CT pulmonary angiography results with objective grading of clinical suspicion.
The sensitivity of CT for VTE improves by combining the CT pulmonary angiography results with objective grading of clinical suspicion.
 The accuracy of CT for diagnosis of PE decreases with poorer scan quality and for smaller and more peripheral clots.
The accuracy of CT for diagnosis of PE decreases with poorer scan quality and for smaller and more peripheral clots.
 Contraindications to CT include contrast allergy, severe renal dysfunction, or inability to safely travel. Patients with a contraindication to CT or inadequate CT results should undergo other testing.
Contraindications to CT include contrast allergy, severe renal dysfunction, or inability to safely travel. Patients with a contraindication to CT or inadequate CT results should undergo other testing.
 Negative d-dimer and multidetector chest CT tests exclude most PE.
Negative d-dimer and multidetector chest CT tests exclude most PE.
 Advantages of CT scan over V/Q scan include more diagnostic results (positive or negative), fewer indeterminate or inadequate studies, and the detection of alternative or concomitant diagnoses, such as dissecting aortic aneurysm, pneumonia, and malignancy.
Advantages of CT scan over V/Q scan include more diagnostic results (positive or negative), fewer indeterminate or inadequate studies, and the detection of alternative or concomitant diagnoses, such as dissecting aortic aneurysm, pneumonia, and malignancy.
• V/Q scan is useful for diagnosis in correlation with pretest probability and can be used in patients with contraindications or indeterminate readings from a PE protocol CT.15
 V/Q scanning remains most useful in a patient with a normal CXR, because nondiagnostic V/Q scans commonly occur in the setting of an abnormal CXR.
V/Q scanning remains most useful in a patient with a normal CXR, because nondiagnostic V/Q scans commonly occur in the setting of an abnormal CXR.
 V/Q scans may be classified as normal, nondiagnostic (i.e., very low probability, low probability, intermediate probability), or high probability for PE.
V/Q scans may be classified as normal, nondiagnostic (i.e., very low probability, low probability, intermediate probability), or high probability for PE.
 Use of clinical suspicion improves the accuracy of V/Q scanning. A normal or low probability V/Q scan in the setting of a low clinical suspicion adequately rules out PE. A high probability V/Q scan in the setting of a high clinical suspicion adequately confirms PE and no further testing is warranted.
Use of clinical suspicion improves the accuracy of V/Q scanning. A normal or low probability V/Q scan in the setting of a low clinical suspicion adequately rules out PE. A high probability V/Q scan in the setting of a high clinical suspicion adequately confirms PE and no further testing is warranted.
 In the setting of an indeterminate result, further testing should be done.
In the setting of an indeterminate result, further testing should be done.
• Venous compression ultrasonography (CUS) is an easily accessible diagnostic modality that can act as a surrogate test for PE if it detects lower extremity proximal DVT and the clinical scenario is highly suggestive of PE.
 Lower extremity venous CUS is not a first-line modality unless the above testing is not available or indeterminate.
Lower extremity venous CUS is not a first-line modality unless the above testing is not available or indeterminate.
 If CUS does not detect DVT and clinical suspicion for PE is high, further diagnostic testing should be performed.
If CUS does not detect DVT and clinical suspicion for PE is high, further diagnostic testing should be performed.
• Echocardiography may assess cardiopulmonary reserve and evidence of end-organ damage (RV dysfunction) in patients with PE and has a role in decision-making regarding the use of thrombolytic therapy.16–18
 Echocardiography may detect a right heart thrombus or visualize an embolism in transit.
Echocardiography may detect a right heart thrombus or visualize an embolism in transit.
 Findings that suggest PE include RV dilation and hypokinesis; increase in RV/left ventricular (LV) diameter ratio; pulmonary artery dilation; tricuspid regurgitation; paradoxical septal motion; interventricular septal shift toward the LV; and McConnell sign, defined by hypokinesis of the free wall of the RV with normal motion of the apex.
Findings that suggest PE include RV dilation and hypokinesis; increase in RV/left ventricular (LV) diameter ratio; pulmonary artery dilation; tricuspid regurgitation; paradoxical septal motion; interventricular septal shift toward the LV; and McConnell sign, defined by hypokinesis of the free wall of the RV with normal motion of the apex.
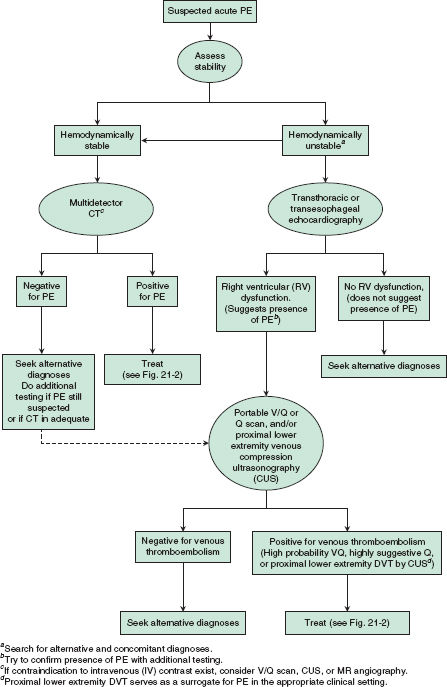
FIGURE 21.1. Diagnostic evaluation for suspected acute pulmonary embolism (PE). (From Otepka HC, Yusen RD. Pulmonary embolism. In: Kollef M, Isakow W, eds. The Washington Manual of Critical Care. 2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2013:97–104.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


