After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with pulmonary edema. • Describe the causes of pulmonary edema. • List the cardiopulmonary clinical manifestations associated with pulmonary edema. • Describe the general management of pulmonary edema. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. Pulmonary edema results from excessive movement of fluid from the pulmonary vascular system to the extravascular system and air spaces of the lungs. Fluid first seeps into the perivascular and peribronchial interstitial spaces; depending on the degree of severity, fluid may progressively move into the alveoli, bronchioles, and bronchi (see Figure 19-1). Movement of fluid in and out of the capillaries is expressed by Starling’s equation: where J is the net fluid movement out of the capillary, K is the capillary permeability factor, Pc and Pi are the hydrostatic pressures in the capillary and interstitial space, and πc and πi are the oncotic pressures in the capillary and interstitial space. When the hydrostatic pressure within the pulmonary vascular system rises to more than 25 to 30 mm Hg, the oncotic pressure loses its holding force over the fluid within the pulmonary capillaries. Consequently fluid starts to spill into the interstitial and air spaces of the lungs (see Figure 19-1). Clinically, the patient with left ventricular failure often has anxiety, delirium, dyspnea, orthopnea, paroxysmal nocturnal dyspnea, cough, fatigue, and adventitious breath sounds. Because of poor peripheral circulation, such patients often have cool skin, diaphoresis, cyanosis of the digits, and peripheral pallor. Increased pulmonary capillary hydrostatic pressure is the most common cause of pulmonary edema. Box 19-1 provides common causes of cardiogenic pulmonary edema. Box 19-2 provides common risk factors for coronary heart disease (CHD).
Pulmonary Edema
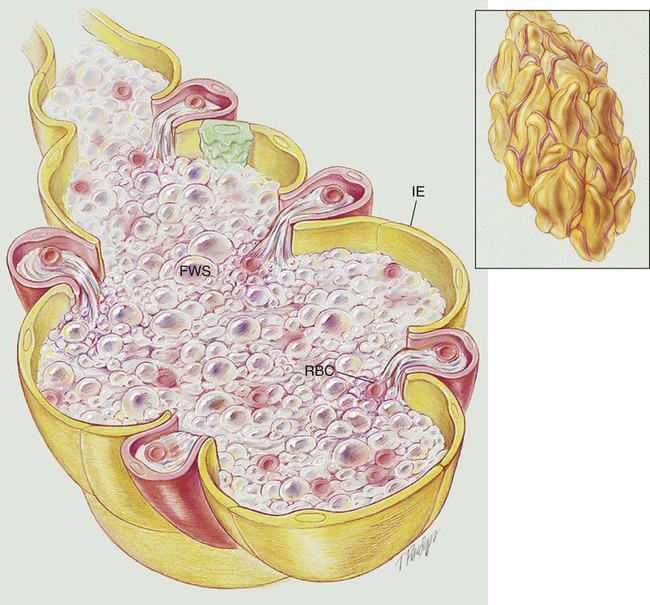
Anatomic Alterations of the Lungs
Etiology and Epidemiology
Cardiogenic Pulmonary Edema

Noncardiogenic Pulmonary Edema
Increased Capillary Permeability
Pulmonary Edema