Advances in CT technology over the past few decades have let to improvements in both spatial and temporal resolution. Most modern multidetector CT (MDCT) scanners can provide isotropic voxel sizes of <1 cm, and even newer scanners can image patients with isotropic voxels of 0.5 mm. In addition, the temporal resolution of most modern MDCT scanners is <300 ms, and newer technologies allow for effective temporal resolutions as low as 66 ms.1 This rapid temporal resolution can be paired with dual-source (two x-ray tubes) or long z-axis (256 to 320 slices) technology to allow for acquisition of the entire chest in <3 seconds and in some instances in <1 second. These advances in both spatial and temporal resolution allow for accurate assessment of both the lung parenchyma and distal airways at radiation doses <1 mSv.2
As the CT scanner emits photons, these particles are attenuated as they travel through the patient before reaching the detectors on the other side of the scanner. Various types of material will attenuate the beam in different ways, and these differences are manifest as grayscale images. For instance, photons easily travel through air and appear black, while metal blocks nearly all photons and will appear white. This attenuation has a scale called Hounsfield units (HU), which, although relatively standardized, can demonstrate some degree of variability depending on the scanner type, kilovoltage used, and scan image parameters such as slice thickness and kernel of reconstruction. According to the scale, water is set at 0 HU and air is set at -1,000 HU. There are no upper limits of attenuation. Fat, which attenuates fewer photons than water but more than air, has an HU around -100 HU, and soft tissue (muscle, solid organs, etc.), which attenuates more photons than water but less than bone, has an attenuation value that can range from 40 to 100 HU. Bone metal attenuates the most photons and appears relatively white.
Glossary of Selected Radiologic Terms
Nodules and Masses
The only difference between a nodule and a mass is size. A nodule is a focal opacity measuring up to 3 cm in diameter, and a mass is a lesion measuring >3 cm in diameter.3 Nodules and masses can be rounded, lobulated, speculated, or poorly defined. Current terminology suggests the division of nodules into two main categories, solid and subsolid. Subsolid nodules can be composed of only ground-glass attenuation (Table 10.1) or be composed of both solid and ground-glass component. A nodule is a nonspecific finding and can be seen in numerous disease states ranging from inflammation to malignancy (Table 10.2). Although most nodules found on CT are benign, follow-up imaging is often necessary to assess for changes over time.
TABLE 10.1 Causes of Diffuse Ground-Glass Opacity
Acute
Subacute to Chronic
Pulmonary edema
Organizing pneumonia
Pulmonary hemorrhage
Hypersensitivity pneumonitis
Infections
Infections
Pneumocystis pneumonia
Pneumocystis pneumonia
Cytomegalovirus pneumonia
Herpes simplex pneumonia
Diffuse alveolar damage, exudative phase
Diffuse alveolar damage, organizing and fibrotic phases
Acute respiratory distress syndrome
Acute interstitial pneumonia
Acute eosinophilic pneumonia
Nonspecific interstitial pneumonia
TABLE 10.2 Differential Diagnosis of Pulmonary Nodules
Pinpointing the exact etiology of nodules or masses can be very difficult and relies on size, number, tissue composition and morphology, and distribution. Although size is not a reliable indicator of benignity, in general, the larger a nodule is, the greater the chance of malignancy.4 Nodules measuring <4 mm in diameter have less than a 1% chance of being malignant, while nodules around 8 mm in diameter have a 10% to 20% change of being malignant.5 In terms of likelihood ratio (LR), solitary nodules <1 cm in diameter, nodules between 1.1 and 2 cm, nodules between 2.1 and 3 cm, and masses >3 cm have an LR of malignancy of 0.52, 0.74, 3.67, and 5.23, respectively. Nonetheless, over 90% of nodules measuring <2 mm in diameter are benign.6
The presence of macroscopic fat in a nodule is almost always indicative of a benign tumor, most notably a hamartoma, although ˜50% of hamartomas contain no visible fat on CT. In very rare instances, fat can be seen within malignant lesions, namely primary pulmonary or metastatic liposarcomas.
Most calcified nodules are benign, and there are six patterns of calcification of a pulmonary nodule, including diffuse, central, laminated, “popcorn like,” amorphous, and punctate. Except for amorphous and punctate calcifications, the other patterns of calcification within a nodule or mass suggest that it is benign. Most calcified nodules seen on CT are due to prior granulomatous infection, and one usually sees numerous, small, well-defined calcified nodules. Popcorn-like calcifications can be seen in both hamartomas and amyloidomas. Amorphous or punctate calcifications have no real pattern or distribution with the nodule and appear as single or multiple flecks of calcification with a lesion. This pattern should raise the possibility of malignancy.7
In the case of a solid solitary pulmonary nodule with soft tissue attenuation, a smooth contour and ovoid shape are suggestive of a benign process, while a spiculated or ragged margin and a more complex, nonrounded shape suggests a malignant process (Figs. 10.1 and 10.2). However, there is significant overlap between these findings, and the presence of a smooth, ovoid nodule does not exclude the diagnosis of malignancy. Other findings suggestive of malignancy include vascular convergence, surrounding pleural retraction, and air bronchograms within a nodule. Cavitation can be seen with certain malignancies such as squamous cell carcinoma but can be seen with certain infections, vasculitis, and inflammatory conditions.5 In general, nodules or masses with a thicker cavity wall are more likely to be malignant than those with a thinner cavitary wall.
Subsolid nodules, either pure ground-glass opacity (pGGO) nodules or mixed-solid and ground-glass opacity (mGGO) nodules, are less common than solid nodules but have a higher likelihood of being malignant. However, in non-lung cancer screening situations, short-term follow-up is important as in one study nearly 40% of pGGO and 50% of mGGO nodules resolved or significantly decreased in size on repeat CT performed 3 months later.8 Nodules that persist on follow-up imaging have a high incidence of malignancy with one study demonstrating that 75% of persistent subsolid nodules were in the adenocarcinoma spectrum ranging from adenocarcinoma in situ (AIS) to invasive adenocarcinoma, while another 6% were atypical adenomatous hyperplasia (AAH).9 However, persistent subsolid nodules can also represent focal areas of fibrosis or organizing pneumonia in about 20% of cases.5
In general, it can be difficult to differentiate between these benign and malignant etiologies. With pGGO nodules, growth over time can often be difficult to assess because of the long doubling time of AIS, which can exceed 2 years. Therefore, indicators other than growth, such as the presence of internal air bronchograms, pleural retraction, increasing density, and/or vascular convergence within a ground-glass nodule, assume greater importance in suggesting the diagnosis of a lesion along the adenocarcinoma spectrum.10 Interestingly enough, unlike solid nodules, a rounded shape is more associated with malignancy in subsolid nodules, probably because well-differentiated adenocarcinomas with lepidic growth show relatively little scarring. In some instances, a small solid component may be present if areas of alveolar collapse or fibroblastic proliferation are present. However, any solid component should raise concern for a more invasive lesion. Changes in size and morphology may occur very slowly and require comparison with CT images performed over many years (Fig. 10.3).
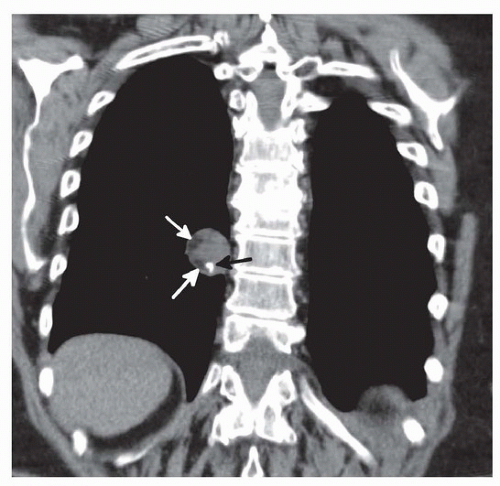
FIGURE 10.1 ▲ Imaging characteristics of a benign lung nodule. Image from a coronal CT obtained in a 69-year-old woman shows a solitary, well-rounded nodule with areas of macroscopic fat (white arrows) and a chunky calcification (black arrow). The findings are diagnostic of a pulmonary hamartoma, which is a benign nodule.
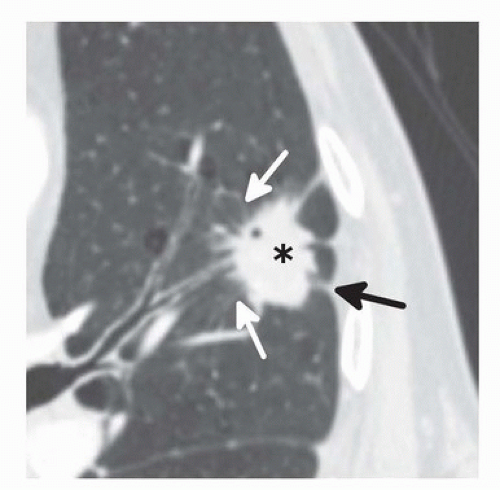
FIGURE 10.2 ▲ Imaging characteristics of a malignant nodule. Axial CT image through the lingual in a 72-year-old man with a long history of smoking shows a 2.4-cm nodule (asterisk). The nodule has a spiculated margin (white arrows) and causes mild retraction of the adjacent pleural surface (black arrow). Close interval follow-up CT showed no change in the lesion, which was subsequently shown to represent a squamous cell carcinoma on biopsy.
Location or nodules can help with determining their underlying cause. For instance, perifissural nodules are most likely benign lymphatic tissue and have an extremely low incidence of malignancy. In three large lung cancer screening studies, of 1,098 perifissural nodules, not a single one was malignant.4,11,12 In terms of lobar location, although lung cancers can occur in any lobe, they are still more common in the upper lobes, on the right greater than the left.4,10 On the other hand, metastatic lesions, which are often multiple, are more common in the lower lobes due to increased blood flow to this area. In addition, metastases tend to be well rounded and located peripherally rather than centrally.
Only gold members can continue reading. Log In or Register to continue