Miscellaneous Carcinomas of the Thymus
Borislav Alexiev, M.D.
Fabio R. Tavora, M.D., Ph.D.
Undifferentiated Thymic Carcinoma
Undifferentiated thymic carcinoma represents between 1% and 27% of thymic carcinomas.1,2,3,4,5,6,7 By definition, these tumors do not fit the criteria for diagnosis of other described subtypes and are undifferentiated carcinomas with solid growth that express at least one epithelial marker (Fig. 111.1).
Distinction from poorly differentiated squamous carcinoma rests on lack of expression of squamous specific markers, such as p40, p63, or cytokeratin 5/6. Distinction from small cell carcinoma rests on histologic features (lack of nuclear molding, stippled chromatin) and lack of diffuse endocrine marker positivity (CD56, synaptophysin, or chromogranin). Rare thymic tumors with rhabdoid features are usually considered as a type of undifferentiated carcinoma or are sometimes considered separately.7
Sarcomatoid Carcinoma
Terminology
Sarcomatoid carcinoma is a thymic carcinoma in which part or the entire tumor resembles soft tissue sarcoma morphologically.8,9,10,11,12,13,14,15 The sarcomatoid component may arise from metaplasia of the carcinomatous component, wherein the tumor cells often gradually lose epithelial characteristics and simultaneously acquire mesenchymal or mesenchymal-like features. Alternatively, the tumor is derived from primitive cells with multidirectional differentiation.
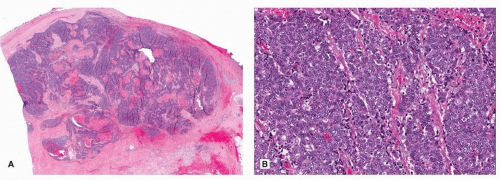 FIGURE 111.1 ▲ Undifferentiated thymic carcinoma. A. Low magnification shows infiltrative tumor with no residual thymus tissue. B. Higher magnification shows undifferentiated carcinoma. Immunohistochemical stains for squamous markers (p63, cytokeratin 5/6) were negative (not shown). |
Incidence and Clinical
Sarcomatoid carcinoma is uncommon and accounts for only up to 7% of all thymic carcinomas.15 It is a tumor of late adulthood, predominantly fourth to eighth decades. No consistent gender predilection has been reported.
Gross Pathology
Grossly, the tumor is unencapsulated, often with infiltrative borders. The cut surfaces show whitish or grayish fleshy tumor with variable extent of necrosis and hemorrhage.15
Microscopic Pathology
Histologically, sarcomatoid carcinoma is an infiltrative tumor often with large areas of coagulative necrosis. It shows intimate intermingling of carcinomatous and sarcomatoid components (Fig. 111.2), but the carcinomatous component can be subtle or demonstrable only by immunohistochemistry or electron microscopy in some cases.15 The carcinomatous component usually comprises cohesive clusters and sheets of poorly differentiated epithelial cells with significant nuclear pleomorphism.8,9,10,11,12,13,14 The sarcomatoid component frequently comprises fascicles and storiform arrays of discohesive spindle tumor cells with
pleomorphic nuclei, coarse chromatin, distinct nucleoli, and frequent mitotic figures. Heterologous elements may be observed, most commonly rhabdomyosarcomatous and occasionally osteosarcomatous; the term “carcinosarcoma” is sometimes applied for such cases.15
pleomorphic nuclei, coarse chromatin, distinct nucleoli, and frequent mitotic figures. Heterologous elements may be observed, most commonly rhabdomyosarcomatous and occasionally osteosarcomatous; the term “carcinosarcoma” is sometimes applied for such cases.15
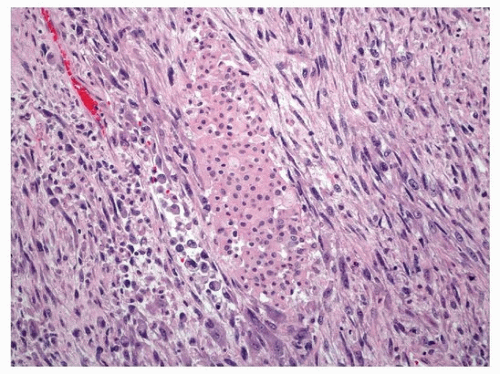 FIGURE 111.2 ▲ Sarcomatoid carcinoma, thymus. Note spindling and focal nests of epithelioid cells. |
Special Studies
Immunohistochemically, the carcinomatous component expresses epithelial markers such as cytokeratin and EMA. In the sarcomatoid areas, cytokeratin-positive tumor cells range from abundant to scanty or even absent.15 Variable expression of myeloid markers (e.g., desmin, actin, myogenin, myoD1, myoglobin) is seen in the rhabdomyosarcomatous component.8,13,15 The cases studied for CD5 have been negative for this marker.15 Only rare tumors have been examined ultrastructurally, but desmosome-like junctions have been described in the spindle cell area of one case.8
Only one case has been studied by cytogenetics, with identification of a complex chromosomal abnormality including der(16)t(1;16) (q12;q12.1).8 This chromosomal translocation has also been previously reported in a case of thymic squamous cell carcinoma, suggesting a pathogenetic relationship with thymic squamous cell carcinoma in at least some cases.
Differential Diagnosis
Sarcomatoid carcinoma may resemble metaplastic thymoma. The former often shows prominent coagulative necrosis, significant cytologic atypia, and readily identified mitotic figures. In a tumor where only sarcomatoid component is identified despite extensive sampling, distinction from a sarcoma depends on the demonstration of epithelial differentiation in at least some tumor cells by immunohistochemistry (cytokeratin, EMA) or electron microscopy. Sarcomatoid carcinoma predominated by rhabdomyosarcomatous component may have been confused with mediastinal rhabdomyosarcoma. The latter sarcoma more commonly affects children and young adults.15 Although rhabdomyosarcoma can express cytokeratin, the positive tumor cells coexpress myeloid markers, whereas at least some tumor cells in sarcomatoid carcinoma express cytokeratin only.8,13
Treatment and Prognosis
Sarcomatoid carcinoma is an aggressive tumor, with frequent invasion of the adjacent pleura, lung, pericardium, and the major blood vessels in the mediastinum. Metastases to mediastinal lymph nodes and parenchymal organs (especially the lungs) are common. Most patients are dying of disease despite aggressive multimodality therapy.15
Clear Cell Carcinoma
Terminology
Clear cell carcinoma is a thymic carcinoma predominantly or exclusively composed of cells with optically clear cytoplasm.15
Incidence and Clinical
Clear cell carcinomas constitute only 3% of all thymic carcinomas.16 The age range of the reported cases is 33 to 84 years, and the tumor tends to prevail in men (male to female ratio, 1:6).15 The patients usually presented with signs and symptoms caused by compression of mediastinal organs, but some patients are asymptomatic and incidentally found to have an anterior mediastinal mass upon imaging examination. There are no associated paraneoplastic autoimmune phenomena.15
Gross Pathology
The tumors may appear encapsulated and noninfiltrative, or may extensively infiltrate the surrounding tissues.15 The cut surface shows solid or cystic tumor with or without hemorrhage and focal necrosis.
Microscopic Pathology
Microscopically, the tumors are composed of cells with clear cytoplasm and rather bland nuclear features and show a lobular, nested, or occasionally sheet-like growth pattern (Fig. 111.3).15,16,17,18,19,20,21,22,23,24,25 Tumor cells are rather monotonous and polyhedral and usually display slight cellular pleomorphism with round to oval, vesicular nuclei, moderate nuclear atypia, finely dispersed chromatin, and small discernible nucleoli. They have abundant lucent, mostly clear to granular, sometimes faintly eosinophilic, cytoplasm. The stroma is fibrotic and lacks the sinusoidal vasculature characteristic of metastatic clear cell carcinoma of the kidney. Rarely, a few scattered intratumoral lymphocytes, minute foci of squamous differentiation, and focal necrosis are observed. Clear cell carcinomas commonly exhibit an infiltrative growth, with tumor extending into the surrounding mediastinal fat and remnant thymus.
Special Studies
Cytoplasmic glycogen is demonstrable in the majority of cases, whereas mucin is absent. The tumor cells are uniformly immunoreactive for low and high molecular weight keratins and are reactive for EMA in 22% of cases.19 As in other types of thymic carcinomas, a subgroup of clear cell carcinomas may express CD5.15 They are negative for PLAP, vimentin, carcinoembryonic antigen (CEA), and S10015,19 and do not contain a population of immature (CD1a- or CD99-positive) T lymphocytes.15
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


