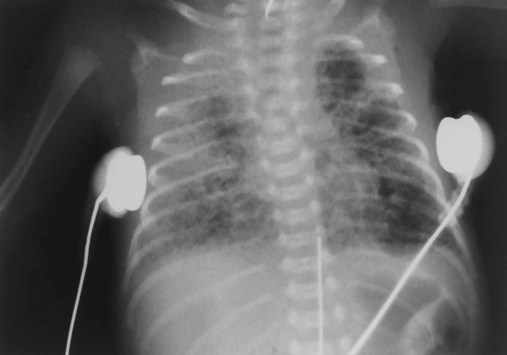
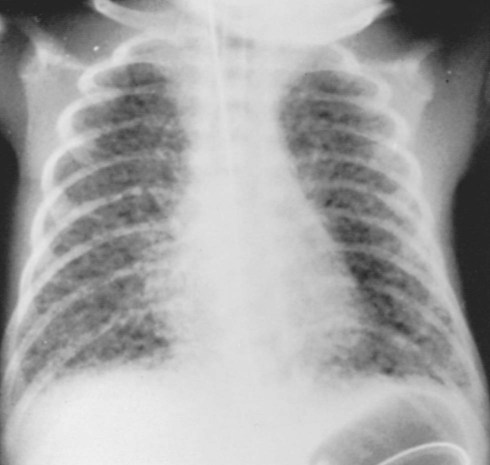
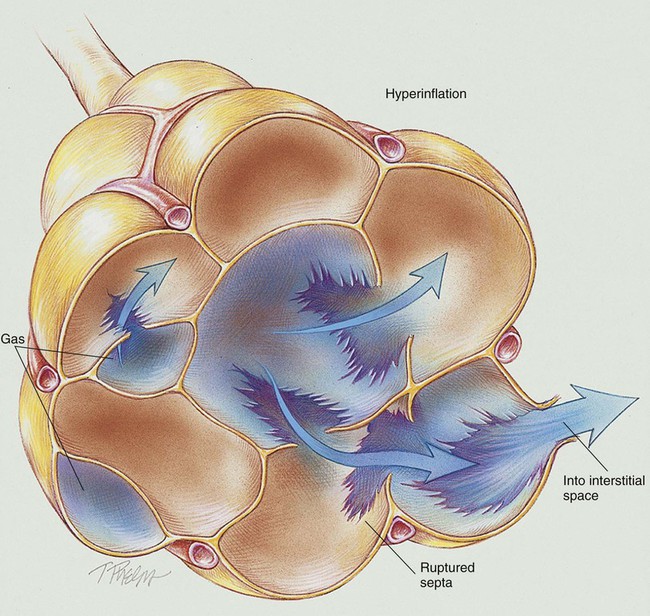
By the end of this chapter, the reader will be able to: • List the anatomic alterations of the lungs associated with pulmonary air leak syndrome. • Describe the causes of pulmonary air leak syndrome. • List the cardiopulmonary clinical manifestations associated with pulmonary air leak syndrome. • Describe the general management of pulmonary air leak syndrome. • Describe the clinical strategies and rationales of the SOAP presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. Pulmonary air leak syndromes (also called air block syndromes) in the infant comprise a large spectrum of clinical entities, including pulmonary interstitial emphysema (PIE), followed by, in severe cases, pneumomediastinum, pneumothorax, pneumopericardium, pneumoperitoneum, and, in rare cases, intravascular air embolism. Pulmonary air leak syndromes are common complications of mechanical ventilation in premature infants, especially when very high pressures are used. They are often seen in infants being treated for respiratory distress syndrome (see Chapter 34). Virtually all pulmonary air leak syndromes begin with some degree of PIE. When high airway pressures are applied to an infant’s lungs (e.g., during mechanical ventilation), the distal airways and alveoli often become overdistended—that is, they develop bleb or emphysema-like areas—and rupture (see Figure 35-1). In addition, gas trapping from an insufficient expiratory time can also cause alveolar overdistention and rupture. Once the gas escapes, it is forced into (1) the loose connective tissue sheaths that surround the airways and pulmonary capillaries, and (2) the interlobular septa containing pulmonary veins. In severe cases, the gas continues to spread peripherally by dissecting along the peribronchial and perivascular spaces to the hilum of the lung, producing the classic radiographic appearance of PIE that shows bubbles of air in the interstitial cuffs (Figure 35-2 and Figure 35-3). A pneumothorax may occur because of the alveolar overdistention and subsequent rupture commonly associated with a PIE (Figure 35-4). A pneumopericardium can develop from direct tracking of interstitial air along the great vessels into the pericardial sac (Figure 35-5). Gas pressure in the pericardium restricts atrial and ventricular filling, resulting in a decreased stroke volume and, ultimately, a reduced cardiac output and systemic hypotension. During the late stages, inflammatory changes of the airways lead to increased capillary leakage and excessive bronchial secretions. The major pathologic changes associated with pulmonary air leak syndromes are as follows: The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8)—the major anatomic alteration of the lungs associated with pulmonary air leak syndromes (see Figure 35-1).
Pulmonary Air Leak Syndromes
Anatomic Alterations of the Lungs
Pulmonary Interstitial Emphysema
Etiology and Epidemiology
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pulmonary Air Leak Syndromes
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pulmonary Air Leak Syndromes