The aim of the present analysis was to evaluate the prognostic impact of different ballooning patterns in patients with Takotsubo cardiomyopathy (TTC). A total of 285 consecutive patients with TTC were included. Clinical characteristics and short- and long-term outcomes were compared between patients with typical apical ballooning (n = 204) and patients with an atypical ballooning pattern including midventricular and basal ballooning (n = 81). Patients with typical apical ballooning were significantly older (73.3 ± 10.2 vs 68.4 ± 10.3 years; p <0.01) and had a higher prevalence of diabetes mellitus (25.5% vs 12.3%; p = 0.02). The initial left ventricular (LV) ejection fraction was significantly lower in case of apical ballooning (41.5 ± 10.4% vs 46.9 ± 10.9%; p <0.01) but recovered to normal values in both groups (58.4 ± 8.0 vs 59.7 ± 7.0; p = 0.25). Although 28-day mortality did not differ significantly (p = 0.10), typical apical ballooning was associated with an increased 6-month (13.4% vs 1.3%; hazard ratio [HR] 10.81, 95% confidence interval [CI] 1.47 to 79.66; p = 0.02) and long-term mortality rates (28.9% vs 14.5%; HR 2.24, 95% CI 1.17 to 4.71; p = 0.02). A landmark analysis which included only patients who survived the first 6 months after the initial event demonstrated similar mortality rates in patients with typical (17.9%) and atypical (13.3%) ballooning (HR 1.36, 95% CI 0.67 to 2.79; p = 0.40). In conclusion, in patients with TTC, typical apical ballooning is associated with more severe LV dysfunction at acute presentation and higher mortality rates within the first 6 months after the initial event. After complete recovery of LV function, prognosis is similar in patients with typical and atypical ballooning patterns.
Takotsubo cardiomyopathy (TTC) is characterized by an acute onset of left ventricular (LV) dysfunction due to regional wall motion abnormalities which are completely reversible within several days to weeks. The first case of TTC was reported in 1990 and exhibited akinesis of the mid and apical segments of the left ventricle with hyperdynamic basal contraction. Since then, this distribution of wall motion abnormalities is considered as the typical TTC ballooning pattern. However, variant forms of abnormal LV contraction have been described in patients with TTC during the past decade including midventricular (akinesis of the mid LV segments with preserved basal and apical function) and basal ballooning (basal akinesis with normal mid and apical contraction). The midventricular and the basal ballooning types are summarized as atypical, reversed, or inverted ballooning patterns. More than 3/4 of patients with TTC present with typical apical ballooning, whereas midventricular (15% to 25%) and basal ballooning (1%) occur less frequently. Because LV dysfunction recovers to normal values within a short period, TTC has been long considered a benign disease. Contrary to this assumption, several recent trials reported substantial mortality rates in patients with TTC and a variety of potential complications particularly during the acute and subacute phase of impaired LV function. Importantly, the extent of LV dysfunction differs significantly depending on the ballooning type. Apical ballooning is associated with akinesis/dyskinesis of large portions of the left ventricle, whereas atypical ballooning patterns involve only a few segments. Therefore, the aim of the present study was to evaluate the prognostic impact of different ballooning patterns by comparing short- and long-term mortality between patients with TTC with typical and atypical ballooning.
Methods
Consecutive patients with TTC presenting to the University of Leipzig–Heart Center from January 2005 to December 2013 or the University Heart Center of Lübeck from February 2004 to April 2014 were prospectively identified and included in the trial. TTC was diagnosed based on the Mayo Clinic criteria. Coronary angiography was performed in all patients to exclude significant obstructive coronary artery disease (>50%) or evidence of acute plaque rupture. Furthermore, all patients underwent left ventriculography to determine the ballooning patterns which were defined as follows:
- 1)
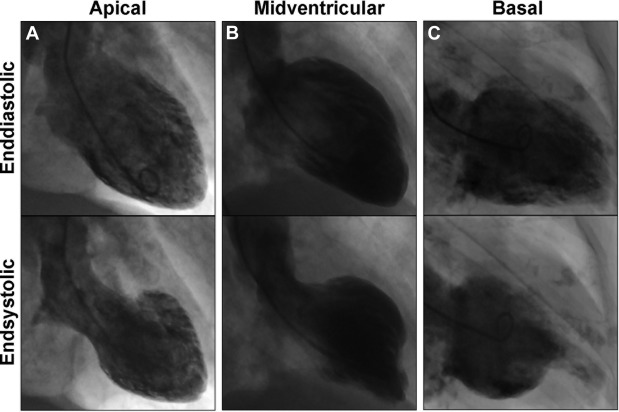
apical ballooning: akinesis/dyskinesis of apical and mid LV segments with preserved basal function;
- 2)
midventricular ballooning: akinesis/dyskinesis of mid LV segments with normal apical and basal function; and
- 3)
basal ballooning: akinesis/dyskinesis of basal LV segments with preserved mid and apical function.
Sample illustrations for the 3 types of contraction patterns are given in Figure 1 . Apical ballooning was considered as typical TTC, whereas patients with midventricular or basal ballooning were categorized as atypical TTC. Cardiovascular magnetic resonance was performed in patients without contraindication presenting to the University of Leipzig–Heart Center to confirm TTC. The standardized protocol included steady state–free precession, T2-weighted, and early and late gadolinium enhancement imaging. A total of 25 patients with suspected TTC were not included in the study because of cardiovascular magnetic resonance evidence of myocarditis or acute myocardial infarction with spontaneous lysis of thrombus. Normalization of LV function within 6 months after the initial event was documented during an outpatient visit.
The study was approved by the institutional review committee and complied with the principles of the Helsinki Declaration. All patients provided informed consent.
Mortality rates were assessed at 28 days and 6 months after the initial event and at long-term follow-up (defined as the time from initial presentation until the last medical contact). The clinical course was documented during regular visits at the institutions or with a structured telephone interview. All events were recorded in standardized case report forms, verified through medical records and contact with the treating physicians and finally adjudicated by experienced cardiologists. Deaths due to myocardial infarction, heart failure, arrhythmia, cerebrovascular disease, pulmonary embolism, and other vascular diseases and sudden cardiac death were classified as cardiovascular deaths. Any death not covered by these definitions was defined as noncardiovascular or death of unknown cause if information concerning the circumstances of death was not available.
Clinical characteristics and mortality rates were compared between patients with typical and atypical ballooning. Continuous variables are reported as mean ± standard deviation and compared with the independent samples t test. Categorical variables are expressed as the number and percentage of patients and compared with the Fisher’s exact test. Hazard ratios (HR) and corresponding 95% confidence intervals (CI) were calculated for outcome data. Moreover, mortality rates were illustrated with Kaplan–Meier plots and compared with the log-rank test. A landmark analysis was performed which included only patients who survived the first 6 months after the initial event. Predictors of 6-month mortality were evaluated with Cox regression analysis. Only significant predictors in univariate analysis were included in multivariate analysis. A 2-sided probability value <0.05 was considered statistically significant. All statistical analyses were performed with SPSS (version 17.0; SPSS Inc., Chicago, Illinois).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


