Lysosome-associated membrane protein (LAMP2) cardiomyopathy is an X-linked and highly progressive myocardial storage disorder associated with diminished survival, which clinically resembles sarcomeric hypertrophic cardiomyopathy. As shown here in a young woman, the natural history of LAMP2 may demonstrate an extreme profile of left ventricular remodeling with regression of hypertrophy (i.e. marked wall thinning), chamber dilatation, and severe systolic dysfunction, all of which are associated with widespread transmural scarring.
Mutations in the X-linked lysosome-associated membrane protein gene (LAMP2) result in a storage disease known as LAMP2 cardiomyopathy, a morphologic phenocopy of sarcomeric hypertrophic cardiomyopathy. LAMP2 mutations are associated with a particularly adverse natural history and a clinical course characterized by progressive (often abrupt) deterioration, with heart failure and malignant ventricular tachyarrhythmias. Of 7 young patients with LAMP2 cardiomyopathy in a recent report, 6 died and/or required heart transplantation before 25 years of age. The unique events documented in the seventh and remaining patient, now 24 years old (and the only female patient), are the subject of this report.
Case Report
Although the patient experienced an appropriate defibrillator intervention for rapid sustained ventricular tachycardia (222 beats/min) at 18 years of age, she remained asymptomatic until 23 years of age, when she experienced an abrupt deterioration in functional state (requiring several admissions for heart failure) due to profound left ventricular (LV) remodeling.
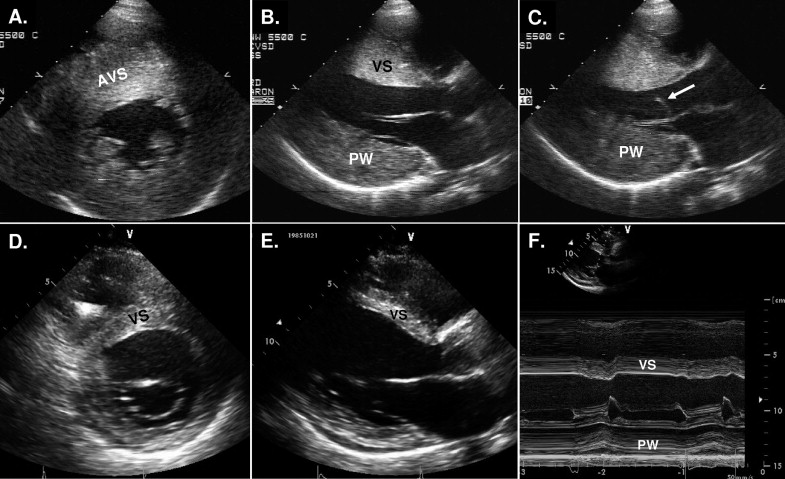
This process showed a more rapid evolution and began earlier in life than is typical of the end-stage phase of sarcomeric hypertrophic cardiomyopathy, involving a striking decrease in LV wall thickness from 30 to 13 mm (a 57% change). There was also an increase in transverse LV cavity dimension from 38 to 60 mm (a 57% change), loss of mitral valve systolic anterior motion, and a reduction in the ejection fraction from 70% to 17% (a 76% change) ( Figure 1 and Table 1 ). The 12-lead electrocardiographic pattern also changed markedly, with striking reductions in precordial and standard lead voltages ( Figure 2 ).
| Parameter | Initial Evaluation | Most Recent Evaluation |
|---|---|---|
| Age (years) | 13 | 24 |
| Ventricular septal thickness (mm) | 30 ⁎ | 13 |
| LV end-diastole (mm) | 38 | 60 |
| Left atrium (mm) | 36 | 34 |
| Ejection fraction (%) | 70 | 17 |
| Cardiac index (ml/min/m 2 ) | — | 1.1 |
| SAM | Moderate † | 0 |
| Electrocardiographic findings | Diffuse T-wave inversion, increased voltages (precordial R wave, 80 mm) | Diffuse T-wave inversion, decreased voltages, intraventricular conduction block (QRS duration 132 ms) |
| NYHA functional class | I | IV |
| Symptoms | Syncope × 2 | Exertional and rest dyspnea, chest pain and fatigue, PND, acute heart failure × 2 |
| Drugs | None | Furosemide, lisinopril, metoprolol |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


