The advances in the detection and management of cardiovascular diseases (CVDs) since the 1960s have resulted in a highly significant age-adjusted decrease in CVD and coronary heart disease (CHD) mortality in men during the past 15 years; an improvement not seen in women, possibly because of the increase in smoking (1). Despite the advances, CVD and CHD still account for more than 50% of deaths and are the most common cause of disability in the Western world. The total burden of CVD in the United States in 2005 was 80.7 million (37%) men and women, and 869.7K died of CVD in 2004 (1). An estimated 16 million in the United States have established CHD. The majority of patients with newly diagnosed CHD present with an acute coronary syndrome (ACS) including unstable angina, myocardial infarction, or sudden death. In 2008 an estimated 770,000 Americans will have an ACS and an additional 190,000 will have a silent first event (1).
Observational studies and randomized trials provide evidence that lifestyle changes and drug therapies can reduce coronary events, strokes, and mortality rates in asymptomatic men and women (2). Clearly, if CHD can be detected in the preclinical stage and a high percentage of those destined for an acute event can be identified by risk stratification, a considerable amount of the related disability and death is preventable. Effective coronary disease prevention requires five major steps: (a) a society willing to pay for prevention, (b) accurate knowledge of the pathobiology of atherosclerosis, (c) an understanding of the contributing risk factors and risk markers, (d) a method of reliable risk stratification or early detection, and (e) safe and effective therapy for risk factors and preclinical disease.
COST AND BENEFIT TO SOCIETIES AND INDIVIDUALS
General agreement exists that societal health care costs can be reduced by prevention and possibly by early detection. It is difficult to measure the cost and relative value of prevention, particularly in CVD. In contrast to preventing communicable diseases such as smallpox and polio, the rationale for using government resources to prevent diseases (e.g., CHD or stroke) that do not threaten the life of others, that may never be manifest, and that, if manifest, do so only in old age requires a considerably different mindset.
Health care costs can be expressed as cost per quality-of-life (QoL) year saved. In the United States, a treatment costing up to $40,000 per QoL-year saved, which is the annual cost for hemodialysis in end-stage renal disease, is considered reasonable, and more than $75,000 per QoL-year, excessive. Although this is a reasonable way to compare the cost of the care provided, known as “direct care,” the method sorely underestimates the value of prevention of atherosclerotic vascular diseases. Equally important are the indirect societal costs of disability from MI, angina, heart failure, and stroke, including lost wages, the cost of medical disability, and the decrease in business productivity. The direct costs of CVD care are in excess of $180 billion dollars, but the total annual economic burden for CVD exceeds $300 billion (1).
The cost expressed as QoL-year saved is influenced by the cost of the drug or treatment, by age, and by the probability of an event’s occurring without treatment. The cost per QoL-year saved by using statins to lower cholesterol levels varies from $15,000 cost saving in persons with established CVD to $150,000 for primary prevention, depending on the expected clinical event rate, age, and gender. The cost of treating healthy men and women who have an estimated annual risk of CHD of 1.5% (intermediate risk) with a generic statin is about $15,000 for each QoL-year saved (3). In comparison, the cost of CHD prevention with aspirin is about $3,000 for each QoL-year saved; and for treatment of hypertension in middle-aged men and women, from less than $5,000 to more than $300,000, depending on the drug (4). What is not considered in the cost analysis is that CV events are not necessarily avoided but rather delayed, and the cost of other medical conditions in survivors, including dementia and cancer, is not factored as future expense. Regardless of the cost and who pays (patient, third party, health maintenance organization), guidelines are needed to provide a method of selecting who would benefit from treatment according to an estimate of individual risk of the disease being prevented, the likelihood of success of the treatment, and a cost-benefit assessment.
PATHOBIOLOGY OF ATHEROSCLEROSIS
Atherosclerosis is a systemic vascular disease involving the aorta and the coronary, carotid, and peripheral arteries. It is the result of inflammation in response to endothelial injury by one or more risk factors, such as hypertension, oxidized low-density lipoprotein (LDL), smoking, and infection (5). The earliest lesions, fatty streaks, are found in some children and in all men and women between the ages of 15 and 34 years who die of noncardiac causes. Diffuse nonocclusive coronary plaque has been found in 25% to 50% of young people at postmortem examination and by intravascular ultrasonography (6,7), and the amount of fatty streaks and plaque correlates with the prevalence of classic coronary risk factors (6).
At least six major processes occur in the development of atherosclerotic plaque (atheroma), and each is a potential therapeutic target: (a) injury of the endothelial lining, which facilitates entry of monocytes and adherence of platelets and microthrombi that release growth factors; (b) active and passive transport of LDL and very low density lipoprotein (VLDL) remnant particles into the subendothelial space, followed by lipid peroxidation; (c) conversion of monocytes to macrophages that ingest oxidized LDL and transform to lipid-engorged foam cells that coalesce into fatty streaks; (d) inflammatory T-lymphocyte response and release of cytokines and chemotactic proteins that stimulate smooth muscle cells to migrate to the intimal layer and convert from contractile to secretory function; (e) smooth muscle cells and fibroblasts, which provide a matrix skeleton of collagen, fibrin, and calcification; and (f) spontaneous death or digestion of foam cells with release of cholesterol and other lipids to form a lipid pool (5,8).
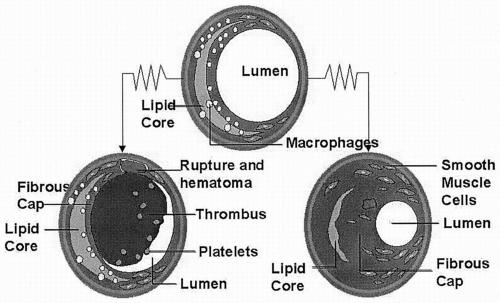
Histologic evidence suggests that plaque growth may be gradual over years, with bursts of growth from periodic intraplaque hemorrhage and repair. The predominant type of plaque in individuals is a major determinant of risk of acute coronary events (8,9). Figure 7.1 demonstrates the two extremes of plaque morphology. Angina pectoris and stress-induced ischemia are usually caused by flow-limiting, partially occlusive, stable coronary stenosis (greater than 70% narrowing) composed of fibrocalcific plaque abundant in smooth muscle and fibrous tissue with or without a lipid pool. Both clinical and pathologic evidence suggests that most acute coronary events are the result of an occluding or partially occluding thrombus at the site of a vulnerable plaque in nonocclusive (less than 70% of vessel diameter) coronary segments (9). The vulnerable plaque has a large lipid pool and a thin fibrous cap that can rupture, often at the junction of the plaque and normal wall, which results in unstable angina, MI, and sudden death (9).
FIGURE 7.1. Progression of the atherosclerotic plaque.
Calcification is uniformly present in early and mature plaque and begins in the second and third decades (10). The calcium is present as a hydroxyapatite identical to that found in bone. A highly significant relation exists between calcium plaque area and atherosclerotic plaque area as measured histologically, and calcium accumulation is more prevalent in complex plaques that may have undergone rupture and healing (11). As with other factors associated with atherosclerosis and the response-to-injury hypothesis, it is highly likely that the amount of calcification of plaque is regulated or influenced by several related and unrelated genes.
The arterial endothelium provides a protective vascular barrier and produces a wide variety of peptides involved in regulating vascular tone, thrombosis, and cellular adhesion, migration, and growth. Nitric oxide (NO·) and prostacyclin are released in response to wall shear stress and autonomic tone (12). Prostacyclin, acting through the cyclic adenosine monophosphate (AMP) pathway, and NO·, acting through the cyclic guanidine monophosphate pathway, are vasodilators with antithrombotic, antiplatelet, antiproliferative, and antioxidant functions. The formation and release of prostacyclin and NO· by the endothelium is impaired in all stages of coronary atherosclerosis in conduit vessels with or without plaque and in the intramyocardial resistance vessels. Impairment of endothelial function is not merely a surrogate for preclinical atherosclerosis. It occurs at all ages simply in the presence of risk factors. Impairment of brachial endothelial function is found in young healthy people with a family history of CHD, in smokers, and in patients with depression, and can be reversed with simple measures (13,14,15,16).
Coronary artery plaque appears focal on angiography but appears diffuse when assessed with intravascular ultrasonography (17). Coronary arteriograms are luminograms and often appear normal in patients with significant arterial wall plaque. The normalization of the lumen in the segments with plaque is the result of arterial enlargement and remodeling (the Glagov effect), which has been demonstrated on pathologic specimens and by intravascular ultrasonography (18,19).
RISK FACTORS AND RISK MARKERS
Coronary risk factors (CRFs) are defined as factors whose presence is associated with or is correlated with an increased likelihood that disease will be present at a later time (20,21). The test of whether a given factor is independent of others and causative generally requires a graded response [e.g., level of LDL cholesterol (LDL-C), tobacco], time exposure (decades), and a response to treatment in placebo-controlled trials (hypertension, cholesterol). However, controlled trials are not always possible or necessary. Observational studies provide adequate evidence of the benefits of smoking cessation, exercise, and weight control. A recent very large international study (nearly 30,000 cases and controls) known as INTERHEART found that the potentially modifiable risk factors associated with a myocardial infarction did not differ by ethnicity or country of origin (22). The surprise was the relative comparability of risk attributable to smoking, lipids, and psychosocial factors and the protective effect of fruits and vegetables, alcohol, and physical activity.
Family history of premature CHD is a major risk factor, but the mechanism is usually illusive or multifactorial. Seventy-five percent of the CHD risk attributed to family history may relate to lifestyle factors, including smoking, diet, obesity, and physical inactivity. Evidence also indicates a strong interaction between genetic polymorphisms and the risk attributable to lifestyle. An example is the gene encoding for aldosterone synthase, in which the C allele is associated with increase in left ventricular mass. Although the C allele has only a modest effect on MI risk, its presence markedly increases the relative risk of MI among smokers and persons with low levels of high-density lipoprotein cholesterol (HDL-C) (23). The weight or contribution of the established major risk factors (particularly LDL-C and HDL-C) creates difficulty in establishing causality for other putative risk factors, which may not have adequate prevalence for detection.
Risk factors can be divided into three major categories: (a) causal, (b) conditional, and (c) predisposing (21). The major clinically useful risk factors are listed in Table 7.1.
Causal risk factors include smoking, hypertension, diabetes mellitus, high total cholesterol (TC) and LDL-C, and low HDL-C. Each factor can be considered to have a continuum of risk from an optimal value (e.g., LDL-C less than 100 mg per deciliter and blood pressure lower than 120/80 mm Hg, with risk increasing for every unit, quartile, or decile), can be considered a categoric risk (e.g., smoking or not), or can be defined by a cut point (e.g., LDL-C higher than 160 mg/dL or blood pressure higher than 140/90 mm Hg). The incremental risk for a factor varies across a wide range of values and is markedly affected by years of exposure and associated risk factors. For example, the risk attributable to LDL-C increases twofold when the triglyceride levels exceed 200 mg per deciliter. The presence of each major risk factor increases the probability of developing CHD about twofold. When several factors are present, the risk may increase 15- or 20-fold. Observational studies suggest that clinically relevant atherosclerosis is unlikely to occur with very low levels of LDL-C, but once the level of LDL-C reaches a “permissive” level and plaque formation begins, the other risk factors independently accelerate plaque formation and instability (21). Diabetes is a particularly strong risk factor, possibly because of its association with other risk factors such as hypertension, low HDL-C, small LDL particle size, and increasing triglyceride levels. The risk for coronary events in diabetic patients without CHD is equivalent to that in men and women with a history of MI (2% or higher annually) (24).
Conditional risk factors [e.g., psychosocial (depression, stress, low locus of control), homocysteine, C-reactive protein, lipoprotein (a), and insulin] are associated with an increased risk for CHD, but the causal link to CHD is uncertain. The uncertainty may be due to their having less influence than the major risk factors, their low frequency, or a required interaction with other factors that is yet unknown. Strong evidence exists in support of the conditional risk factors listed in Table 7.1.
TABLE 7.1.Established and putative coronary risk factors and markers
Predisposing risk factors related to and increasing causal risk
Age: duration of exposure to LDL-C, hypertension, diabetes
Male gender: decrease in HDL-C in comparison with women
Menopause: loss of protective effect of estrogens
Family history of premature CHD: first-degree relative: male <55 yr, female <65 yr
Socioeconomic: hypertension, diet, physical inactivity, less education, low income
Predisposing risk factors generally intensify causal risk factors or conditional risk factors and may be independent and causal but in unidentified ways (e.g., family history, marital status, ethnicity, education and other socioeconomic factors).
Risk markers identify a person as being at increased risk for coronary events, but they may or may not be risk factors for atherosclerosis. Examples would include microalbuminuria, an elevated C-reactive protein, elevated proinflammatory cytokines, interleukin-6 and the enzyme lipoprotein-associated phospholipase A2. The risk of coronary events is increased with higher levels of C-reactive protein (CRP), an acute-phase reactant produced in the liver in response to inflammatory cytokines, but evidence also indicates that CRP itself may influence plaque stability and growth and may be a risk factor for acute events (25).
RISK STRATIFICATION
The physician, the patient, and the payer need guidelines that provide a balance between efficacy, safety, and cost of each diagnostic tool or treatment. Individual risk stratification has been at the heart of guidelines for lipid-lowering and antihypertensive therapies for the prevention of CVD in the United States (26,27). Risk for cardiovascular events is generally divided into tertiles and presented as 10-year or annual risk. Low risk is defined as a 10-year risk of less than 10% (very low risk, less than 6%), intermediate risk, 10% to less than 20%, and high risk equal to or greater than 20%. Patients with CHD have an approximate 2% annual risk of CV events; thus patients at high risk are considered coronary risk equivalents. Examples of CHD risk equivalents include middle-aged and older adults with diabetes, older men with two or more risk factors, and other sites of vascular disease including a stroke, carotid and peripheral vascular disease, and aortic aneurysm.
The significance of individual or multiple risk factors is expressed with the following terms: absolute risk, relative risk or odds ratio, attributable risk, number needed to treat (NNT), relative risk reduction, and categoric risk.
Absolute risk is the probability of an individual’s developing a defined end point (i.e., coronary event) over a finite period, such as 150 per 1,000 over a 10-year period, or 1.5% annually. For example, by using the Global Risk Score (derived from the Framingham Heart Study) in Table 7.2, the 10-year risk of a coronary event in a 50-year-old man with a cholesterol level of 250 mg per deciliter and no other risk factors is 6%, or 0.6% annually (28).
Relative risk or odds ratio is the ratio of absolute risk in a patient with one or more risk factors in comparison with a person with standard risk. For example, the relative risk for development of CHD over a 10-year period in a 50-year-old man with a cholesterol level of 249 mg per deciliter in comparison with 199 mg per deciliter is 1.5 (odds ratio, 1.5), or 50% greater (28). The relative risk appears high, but the absolute risk for both men is relatively low: 0.6% versus 0.4% annually.
Attributable risk is the additional probability an individual with a risk factor will have an event over time in comparison with the standard risk. In the previous example, the attributable risk of the added 50 mg per deciliter in the 50-year-old man is 20 per 1,000, or 2% for 10 years and 0.2% annually.
Number needed to treat is the number of patients with a given risk factor needed to treat (NNT) to prevent one event over a given period of time; for example, treating 25 subjects for 5 years will prevent one event. This is estimated after a clinical trial in which a treatment group and a control group participate. Values are entered as events per 100 or per 1,000 (expressed as a decimal fraction) in the placebo or standard treatment and new treatment groups [NNT = 1 ÷ (control − treated)]. For example, assume that the hypothetical drug “Atherobloc” reduced the 5-year coronary event rate by 50% in comparison with placebo in 10,000 high-risk patients. The Atherobloc-treated group had 250 events in 5 years or 1% per year; in comparison, the placebo event rate had 500 events or 2% per year. Twenty persons with comparable risk would need to be treated for five years (NNT) to prevent one event.
Relative risk reduction (RRR) is the reduction of adverse events or end points in the treated group versus placebo group in a trial [RRR = (placebo − treated) ÷ placebo].
Categoric risk, or categories of risk, can be expressed in several forms but differ principally from risk when it is expressed as a continuum. A classic categoric-risk method would stratify an individual by a single parameter, such as present or absent (e.g., microalbuminuria, smoking, diabetes); high, intermediate, and low risk; or above or below a numeric cut point (e.g., age, LDL cholesterol, and blood pressure). Several levels of categoric risk are used in the Adult Treatment Panel III (ATP-III) guidelines for cholesterol management (26). The decision for diet, drug therapy, and the LDL-C target goal are based on fasting LDL-C level, the presence of major risk factors (none, one, two, or more), and age and gender.
Prevention decision trees and guidelines have been developed primarily from models based on longitudinal cohort studies and large randomized clinical trials. The Framingham Heart Study, a prospective singlecommunity study of 5,075 people 30 to 74 years of age and without CHD who were monitored for 12 years, provided the evidence for causal risk factors and a frame-work for categoric risk stratification and more complex CHD prediction models (29). The Global Risk Score derived from the Framingham Heart Study (Table 7.2) provides a 10-year estimate of risk for CHD, including the development of stable angina, unstable angina, and fatal or nonfatal MI (28). The weight attributable to the causal independent risk factors in the Framingham Heart Study is similar for white and black men and women (30). For Japanese American men, Hispanic men, and Native American women, the Global Risk Score systematically overestimates the risk of CHD, and overweights the importance of cholesterol in elderly men and women (30). In secondary prevention, short-term risk may encompass 30 days to 6 months, and long-term risk may encompass 5 years. In contrast, in primary prevention, short-term risk encompasses 10 years, and long-term risk encompasses 20 years or a lifetime. The probability of a CHD event occurring in the lifetime of a 40-year-old man is about 40%, and that in a 40-year-old woman is about 25% (31).
TABLE 7.2.Global risk score by Framingham risk estimates
ESTIMATE OF 10-YEAR RISK FOR MEN (FRAMINGHAM POINT SCORES)
ESTIMATE OF 10-YEAR RISK FOR WOMEN (FRAMINGHAM POINT SCORES)
From executive summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497.
Only gold members can continue reading. Log In or Register to continue