Primary hyperhidrosis is the excessive, localised, uncontrollable production of sweat with no discernable cause.
It affects 0.5–1% of the general population with an equal male to female preponderance. Although no true diagnostic definition exists, the condition has been objectively diagnosed gravimetrically as a measured axillary sweat production >50 mg/min.
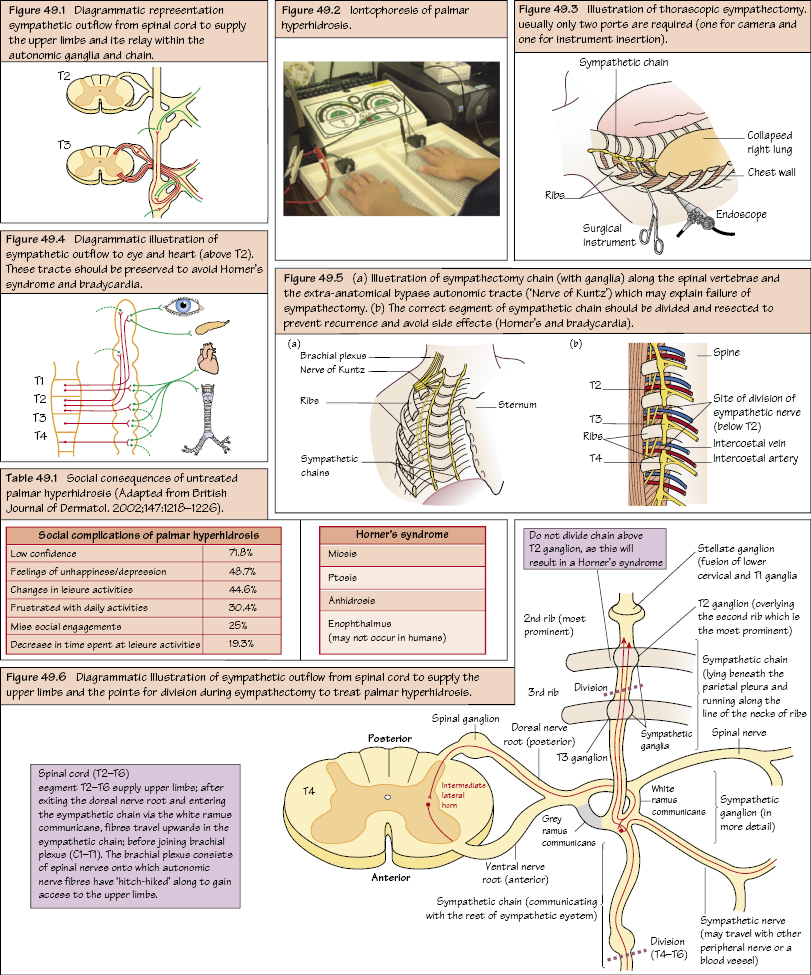
However, if sweating is excessive to the point of having a negative lifestyle effect, then it may be considered problematic to the point of necessitating further treatment (see Table 49.1).
Pathophysiology
Eccrine sweat glands innervated by sympathetic nervous system (SNS).
Uniquely has acetylcholine as neurotransmitter.
Spinal cord segments T2–T6 supply the sympathetic innervation to the upper limbs and passe cephalad to join the brachial plexus.
All postganglionic sympathetic fibres to entire upper limb except axillae run via brachial plexus (C5–T1).
An aberrant (anatomical variant) thoracic origin of the sympathetic supply to the upper limbs may also exist is referred to as the Nerve of Kuntz (variable intrathoracic ramus arising caudal to the normal sympathetic outflow offering an alternative pathway to the upper limbs) This may explain failure or recurrence post-surgical treatment).
Clinical features
Avoid stress triggers and certain foods (e.g. spices, alcohol).
Palms, axillae, soles of feet and, rarely, the entire body.
Patients complain of the social and psychosocial consequences including dripping hands, slippery handgrip, dripping into computer keyboards, embarrassment, offensive odour, wet clothing and depression, as well as the side effects of treatment.
Management
Medical.
Surgical (severe cases where medical management has failed).
Medical Management
Only gold members can continue reading. Log In or Register to continue