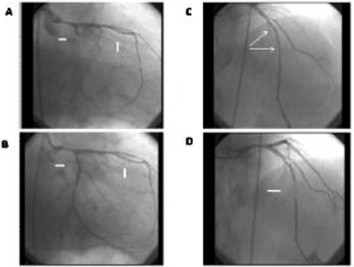
A 70 year-old man presented to the Emergency Department with a 1-hour history crescendo angina that radiating to the left arm and neck. The patient abandoned smoking 10 years ago and had no history of any cardiac disease. Physical examination was unremarkable and the heart rate of 60 beats/min and the blood pressure of 90/60 mm Hg in the emergency unit. The initial ECG demonstrated diffuse ST-segment depression, maximum 2 mm in V-1-2-3.(figure 1). Bedside transthoracic echocardiography (TTE) showed that posterior hypokinesis with a 50% left ventricle ejection fraction(LVEF). After patient’s transfer to coronary angiography laboratory, antiplatelet drugs i.e. 300 mg aspirin and 600 mg clopidogrel were administered. The patient underwent coronary angiography which showed that LAD mid-segment dissection had MB, CX ostial 100% with trombus and right coronary angiography was found normal.
The CX lesion was crossed with a floppy guidewire and then predilated with balloon angioplasty. Then it was observed that CX lesion had dissection. Blood flow of artery of CX was provided by stent implantation (3.0×28-mm everolimus eluting coronary stent,) with a good angiographic result (TIMI-3). Although CX lesion was passed successfully, the patient’s chest pain increased and blood pressure decreased which likely evidence of a LAD dissection and MB. A more detailed evaluation of the LAD in several different projection showed that MB had caused 90% stenosis. We concluded that flow of LAD coronary could be achieved by the second stent implantation and performed it successfully (3.0×38-mm everolimus eluting coronary stent). Normal antegrade flow (TIMI III) of LAD distal to the MB segment without any evidence of dissection is reported(figure 2-3). His hospital course was uneventful and he was discharged with medical treatment( aspirin,clopidogrel, beta-blocker, ACE-I).
Discussion
Spontaneous Coronary Artery Dissection (SCAD) and the Muscular Bridge (MB) are two different coronary events they may come out with the same clinical picture. Accordingly, SCAD may play a role in deaths connected with MB and physiopathogenesis of coronary events. Unfortunately there is no good definition of the optimal management of SCAD and musculer bridge. The choise of therapy should be individualised and in accordance with the extent and severity of SCAD.