Refeeding syndrome is a life-threatening condition occurring in severely malnourished patients after initiating feeding. Severe hypophosphatemia with reduced adenosine triphosphate production has been implicated, but little data are available regarding electrolyte abnormalities. In this case, we report electrocardiographic changes consistent with hyperkalemia during potassium replacement after a serum level increase from 1.9 to 2.9 mEq/L. This was reversed by lowering serum potassium back to 2.0 mEq/L. In conclusion, the patient with prolonged malnutrition became adapted to low potassium levels and developed potassium toxicity with replacement.
Severe fluid and electrolyte disorders are the hallmark of refeeding syndrome. Refeeding syndrome was first recognized during World War II among prisoners in South East Asia and famines in Europe. Here, we report electrocardiographic changes of sinoventricular rhythm, defined as sinus node conduction to the atrioventricular junction without atrial contraction, which occurred at a serum potassium level of 2.9 mEq/L during electrolyte replacement. Such electrocardiographic changes usually occur with hyperkalemia (>8 mEq/L).
Case Description
A 58-year-old severely malnourished Caucasian woman with medical history of hypertension and anxiety disorder presented with a clasped hand and paresthesias. Review of systems revealed a self-imposed starvation secondary to depression. This was associated with a significant recent weight loss of 28 lbs (115 to 87 lbs) per patient. In addition, the patient was taking hydrochlorothiazide without potassium supplement and paroxetine (10 mg/day) but not regularly. By physical examination the patient appeared severely malnourished with a heart rate of 110 beats/min, normal heart sounds, and a clasped right hand. The patient was admitted with the diagnosis of severe electrolyte imbalance, rhabdomyolysis, and malnutrition. Serum potassium, magnesium, and ionized calcium were low ( Table 1 ). The urine was positive for myoglobin, serum albumin was 2.2 g/dl (3.6 to 5 g/dl) and troponin and creatine phosphokinase (CPK) were elevated at 13.93 ng/ml and 4,847 U/L respectively with negative CPK index. Thyroid-stimulating hormone was 4.87 μIU/ml. An initial electrocardiogram demonstrated sinus tachycardia with a prolonged QTc of 535 ms ( Figure 1 ). After admission, the patient became anxious and short of breath. A repeat electrocardiogram was unchanged from the previous one and an echocardiogram revealed ejection fraction of 40%.
| Day | Potassium (3.5-4.9 mEq/L) | Magnesium (1.3-2.1 mEq/L) | Ionized Calcium (1.10-1.30 mmol/L) | Phosphorus (2.5-4.5 mg/dL) | Creatinine (0.60-1.40 mg/dL) |
|---|---|---|---|---|---|
| 1 | 1.9 | 0.6 | 0.71 | – | 0.56 |
| 1 | 2.2 | 2.3 | 0.94 | 2.8 | 0.86 |
| 2 | 2.9 | 1.9 | 1.10 | 1.9 | 0.59 |
| 2 | 2.0 | 1.8 | 1.12 | – | 0.60 |
| 3 | 2.3 | 1.5 | 1.07 | 2.1 | 0.56 |
| 6 | 2.3 | 1.2 | 1.03 | 2.0 | 0.44 |
| 9 | 2.8 | 1.5 | 1.01 | 2.0 | 0.39 |
| 10 | 3.3 | 1.5 | 1.02 | 2.6 | 0.36 |
| 11 | 4.1 | 1.5 | 1.17 | 2.8 | – |
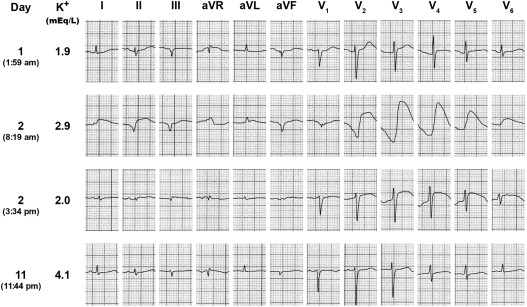
Electrolyte replacement was initiated using a continuous infusion of normal saline containing potassium chloride (20 mEq/L) by the way of a central line at 1.6 mEq/h. During a second infusion of potassium chloride (40 mEq/L) at a rate of 10 mEq/h with magnesium sulfate (4 g) and calcium gluconate (2 g), telemetry demonstrated a widening QRS. A subsequent electrocardiogram demonstrated a life-threatening sinusoidal wave pattern suggestive of hyperkalemia at a serum potassium level of 2.9 mEq/L ( Figure 1 ). These electrocardiographic changes were suspected to be due to a relative hyperkalemia caused by potassium replacement. A decision was then made to lower the serum potassium to previous levels. By giving insulin, oral Kayexalate (sodium polystyrene sulfonate, USP), and calcium gluconate (2 g intravenously), the sinusoidal pattern began to resolve rapidly within 5 to 10 minutes by telemetry and subsequent 12 lead electrocardiogram ( Figure 1 ). Eventually, after oral potassium supplement of 10 mEq KCl, twice daily, magnesium oxide (400 mg/day), and gradual feeding corrected the electrolytes over the next 11 days. The final electrocardiogram demonstrated normal sinus rhythm at 75 beats/min.
The patient was started on lisinopril 2.5 mg/day and metoprolol tartrate 12.5 mg twice daily and discharged home. A repeat echo and Lexiscan (regadenoson) stress test demonstrated normal left ventricular ejection without ischemia or infarction. It was considered that the elevated troponins and CPK were related to the rhabdomyolysis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


