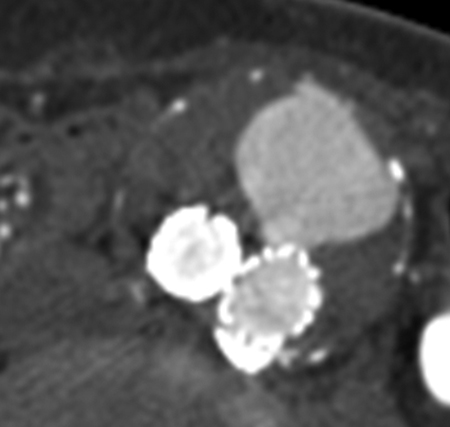
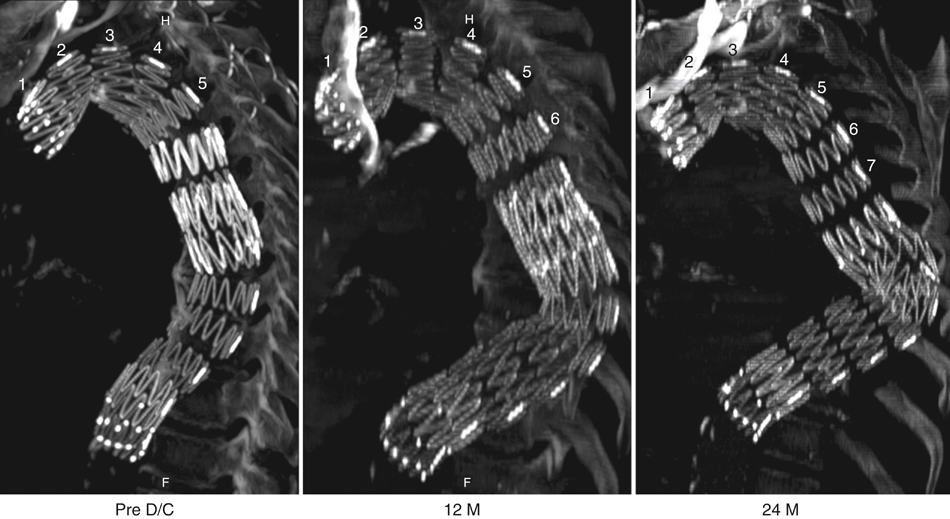
Proper surveillance after endovascular aortic repair shares many features of any postoperative evaluation after a major surgical procedure. In the first postoperative visit, history-taking should focus on fevers and other systemic symptoms, new-onset claudication, hypertension, and azotemia, which could suggest iliac or renovascular compromise. Physical examination should be directed at the groins and other vascular access sites, femoral pulses, and aortic pulsatility in cases of abdominal aortic aneurysms. While pulsatility in isolation is a relatively nonspecific finding, a change from a nonpulsatile to a pulsatile examination during follow-up often indicates a new type I or III endoleak (Figure 1). Any serious access site problems such as infections, seromas, or pseudoaneurysms will manifest themselves within the first 30 days. Unique to endovascular repair are types of imaging that form an integral part of the surveillance regimen. Available imaging modalities include computed tomography angiography (CTA), magnetic resonance angiography (MRA), plain multiview x-ray, duplex ultrasound with or without sonographic contrast, and intrasaccular pressure monitoring. No single modality is sufficient or necessary for each follow-up, and each should be considered complementary depending on the segment of the aorta treated, the pathology, the device’s construction, and the patient’s physiology. The purpose of imaging includes measurement of aortic size and detection of endoleak or device migration (Figure 2) and impaired endograft patency (including kinking and/or compression) and device integrity. Secondary findings include associated vascular problems such as iliac stenosis or dissection, branch vessel compromise or graft infection, and nonvascular pathologies that can masquerade as aortic symptoms and malignancies. Regardless of which modality, any new finding or serial dimensional measurement (e.g., length, distance, diameter) should be compared or performed using the same modality performed the same way, such as aneurysm diameter measured on orthogonal centerline reconstruction.
Postoperative Surveillance of Thoracic and Abdominal Aortic Endografts
Elements of Complete Surveillance
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine