Posterior Compartment Mass
Robert B. Carr, MD
DIFFERENTIAL DIAGNOSIS
Common
Nerve Sheath Tumor
Sympathetic Ganglion Tumor
Lymphoma
Hiatal Hernia
Esophageal Tumor
Less Common
Metastasis
Foregut Duplication Cyst
Extramedullary Hematopoiesis
Aortic Aneurysm
Esophageal Varices
Spine Mass
Rare but Important
Hemangioma
Lymphangioma
Meningocele
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Anatomy of posterior compartment
Description is based upon radiographic landmarks
Anterior border: Line 1 cm behind anterior margin of thoracic vertebrae
Posterior border: Chest wall
Normal contents: Vertebral bodies, descending aorta, azygos vein, esophagus, lymph nodes, adipose tissue
Cervicothoracic sign: Mediastinal mass outlined by lung on frontal radiograph above level of clavicle; indicates posterior location
CT and MR are invaluable for determining site of origin and tissue characterization
Helpful Clues for Common Diagnoses
Nerve Sheath Tumor
More common in adults
Schwannoma, neurofibroma, plexiform neurofibroma
Smooth, round or oval, often less dense than muscle
Enlargement of adjacent neural foramina with occasional extension into spinal canal
Often have internal foci of decreased attenuation due to lipid or cyst formation
Increased signal on T2 MR images and heterogeneous enhancement
Sympathetic Ganglion Tumor
More common in children and young adults
Ganglioneuroma
Benign neoplasm of ganglion cells and Schwann cells
Most common in 2nd and 3rd decades
Calcification in 20%
May have whorled appearance on MR
Ganglioneuroblastoma
Intermediate histology between ganglioneuroma and neuroblastoma
Most common in older children
Imaging resembles neuroblastoma
Neuroblastoma
Malignant neoplasm associated with systemic symptoms
Most common in children less than 5 years old
Curvilinear and speckled calcification in 40%
May invade adjacent structures
Lymphoma
Non-Hodgkin lymphoma is more common than Hodgkin disease in posterior compartment
Enlarged lymph nodes or nodal mass, often displaying homogeneous soft tissue attenuation
Necrosis is occasionally present, usually detected after contrast administration
Hiatal Hernia
Superior herniation of stomach through esophageal hiatus
May see air-fluid level on upright radiograph
Esophageal Tumor
Carcinoma
Thickening of esophageal wall that is often eccentric
Luminal narrowing
Invasion of adjacent tissues
Mesenchymal tumor
Most common histology is leiomyoma
Often asymptomatic
Margins are smooth
Helpful Clues for Less Common Diagnoses
Metastasis
Often involves lymph nodes
Involvement of posterior compartment lymph nodes is suggestive of primary malignancy within abdomen
Foregut Duplication Cyst
Esophageal duplication cyst, bronchogenic cyst, neurenteric cyst
Round or oval with smooth borders
Thin wall with no enhancement; wall calcification is uncommon
Cyst contents may be proteinaceous, with increased attenuation and increased signal on T1 MR images
Neurenteric cysts are associated with adjacent vertebral anomalies
Extramedullary Hematopoiesis
Associated with thalassemia, sickle cell anemia, and spherocytosis
Multiple bilateral paraspinal masses
Sharp borders with homogeneous attenuation
May be associated with skeletal abnormalities
Aortic Aneurysm
May involve aortic arch or descending aorta
True aneurysm: Most commonly due to atherosclerotic disease
False aneurysm: Most commonly due to trauma
Esophageal Varices
Result of liver disease with chronic portal hypertension
Vascular serpiginous masses within middle and posterior mediastinum
Connect with azygos system to bypass portal drainage
Spine Mass
Neoplasms: Myeloma, metastasis, primary bone tumor
Infection: Spondylitis, paraspinous abscess
Look for disc space and vertebral body destruction
If mass is present, determine if it appears to arise from bone or soft tissues
Helpful Clues for Rare Diagnoses
Hemangioma
Soft tissue mass
Clue to diagnosis is internal phlebolith
Appearance similar to soft tissue hemangiomas elsewhere in body
Lymphangioma
Benign hyperplasia of lymphatic vessels
Low-density mass that insinuates between adjacent structures
Meningocele
Herniation of meninges beyond spinal canal
Associated with neurofibromatosis and traumatic nerve root avulsion
Direct communication with subarachnoid space around spinal cord
Associated with adjacent vertebral anomalies in neurofibromatosis
Image Gallery
 Axial NECT shows a soft tissue mass within the posterior mediastinum  that has expanded the right neural foramen that has expanded the right neural foramen  and extends into the central canal and extends into the central canal  . . |
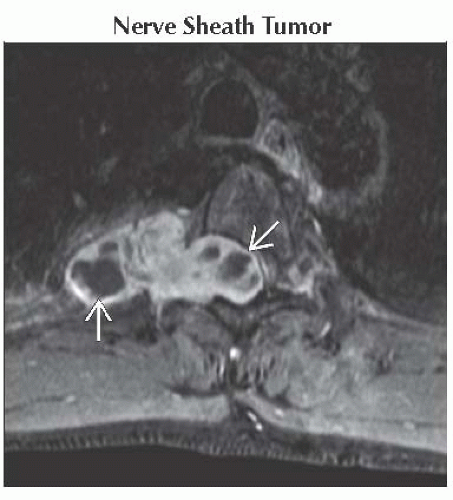 Axial T1WI C+ FS MR in the same patient shows intense enhancement of the mass with several nonenhancing areas  . These areas represent cystic regions, a common finding with schwannomas. . These areas represent cystic regions, a common finding with schwannomas. |
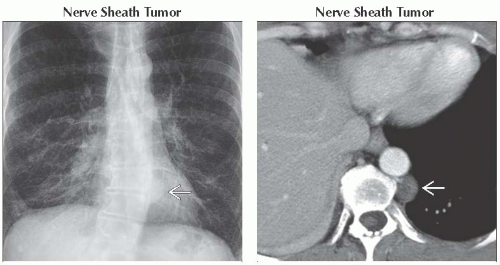 (Left) Frontal radiograph shows mild levoscoliosis and a well-demarcated mediastinal soft tissue mass
 . Note it does not silhouette with the descending thoracic aorta. (Right) Axial CECT in the same patient reveals a round homogeneous mass in the posterior mediastinum . Note it does not silhouette with the descending thoracic aorta. (Right) Axial CECT in the same patient reveals a round homogeneous mass in the posterior mediastinum  . This patient has a history of neurofibromatosis, and this mass is consistent with a neurofibroma. . This patient has a history of neurofibromatosis, and this mass is consistent with a neurofibroma.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|