(1)
Department of General surgery, Fuwai Hospital, Beijing, China
2.1 Position of the Heart
The heart is a muscular organ in the mediastinum, a cavity located anterior to the vertebral column, posterior to the sternum, above the diaphragmatic muscle, and between the two lungs (Figs. 2.1 and 2.2). Its function is to pump blood through the blood vessels by repeated, rhythmic contractions. The portion of interpleural space between the heart and the sternum is called the anterior mediastinum. It contains no important structures and has only a lamellar sternum in front of it; hence, it is the most frequently selected surgical approach to the heart. In contrast is the posterior mediastinum, the interpleural space between the posterior wall of the heart and the vertebral column; it contains many important organs, such as the trachea, the esophagus, the aortic arch, and branches of the descending artery. The trachea branches into two main bronchi on the level of the sternal angle, and enlargement of the LA may raise the left main bronchus. The lower segment of the esophagus is situated close to the posterior wall of the heart. The aortic arch is directed backward on the left side of the trachea and passes downward on the left side of the body. It is also continuous with the descending aorta at the lower border of the fourth thoracic vertebra. A large aortic arch aneurysm may result in dyspnea due to compression of the trachea. The superior mediastinum refers to the cavity located above the heart and between the manubrium sterni and the upper thoracic vertebra. It holds several vital organs, including the thoracic gland, the aortic arch and its vital branches, the anonymous veins, the azygous vein and the upper portion of the SVC, the diaphragmatic nerve, and the vagus nerve. Located behind the heart is the vertebral column.
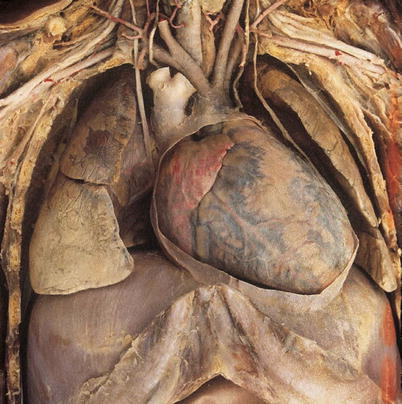

Fig. 2.1
The position of the heart. The heart is located in the mediastinum, anterior to the vertebral column, posterior to the sternum, above the diaphragmatic muscle, and between the two lungs. It is protected by a perfect bony framework
Fig. 2.2
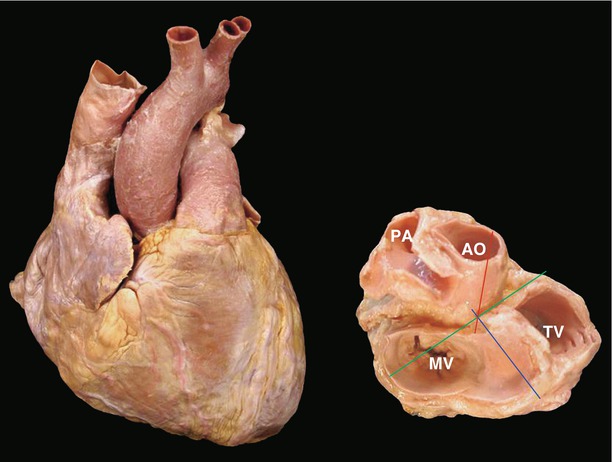
Stereoimaging of the vessels of the heart, lung, and liver
2.2 Observation of the Heart
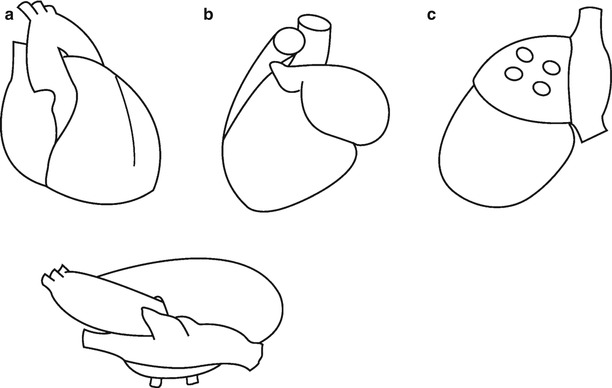
The anatomy of the heart can be described by observing it from different visual angles that provide views of the axes of the heart (Figs. 2.3 and 2.4). The visual angle used most frequently provides a view from the anterior aspect and is called the anatomical angle (Figs. 2.5 and 2.6). The left anterior oblique angle allows the four chambers of the heart to be seen simultaneously (Figs. 2.7, 2.8, 2.9, and 2.10), whereas the right anterior oblique angle provides the clearest visualization of the RA and the RV (Fig. 2.11). Moreover, the operator usually observes the heart from the right shoulder side (Fig. 2.12), so this visual angle may be named the operator angle (Fig. 2.13). In some special conditions, it will be described by some special angles, such as from the side of the head or back (Figs. 2.14 and 2.15).
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Fig. 2.3
The axes of the heart. The blue line parallel to the interatrial septum is the anteroposterior axis; the red line is the cephalocaudal axis; the green line is the Y-axis. These axes cross at the central fibrous trigone. PA pulmonary artery, AO ascending aorta, TV tricuspid valve, MV mitral valve
Fig. 2.4
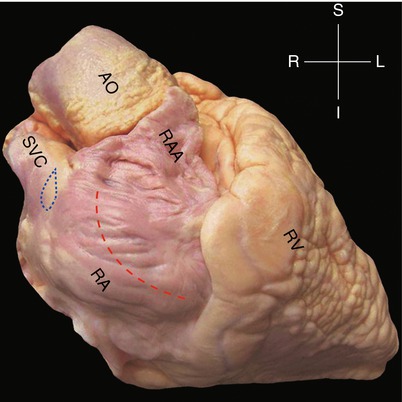
Observation from the anatomical angle. The right atrioventricular groove, with the right coronary artery passing through it, and the anterior interventricular groove, with the left anterior descending artery. The right margin of the heart is composed of the RA, and the inferior margin is formed by the RV. The aortic arch, main pulmonary artery, LAA, and apex constitute the left margin. The red dash line indicates the incision made in the RA during surgery, and the blue dash line indicates the sinoatrial node. AO ascending aorta, RA right atrium, RAA right atrium appendage, RV right ventricle, SVC superior vena cava
Fig. 2.5
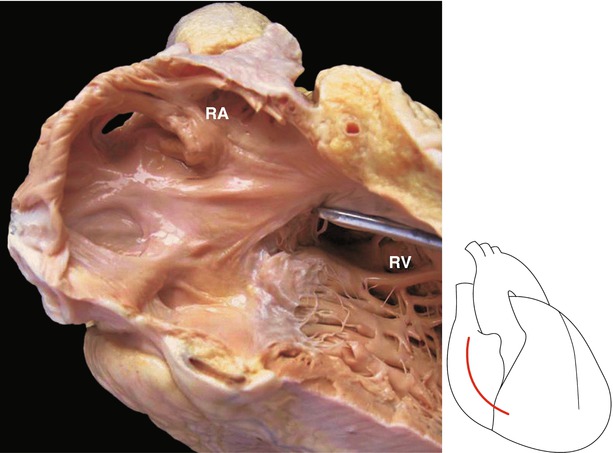
Observation from the right side. Through the RA incision, inner wall of the RA and septal leaflet of the tricuspid valve can been seen. RA right atrium, RV right ventricle
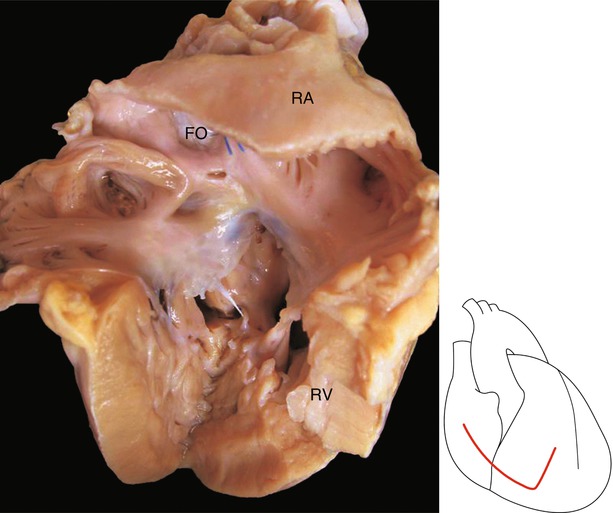
Fig. 2.6
Observation by the right anterior oblique position. The RVOT was exposed. The tricuspid valve and the RA can be seen clearly. FO fossa ovalis, RA right atrium, RV right ventricle
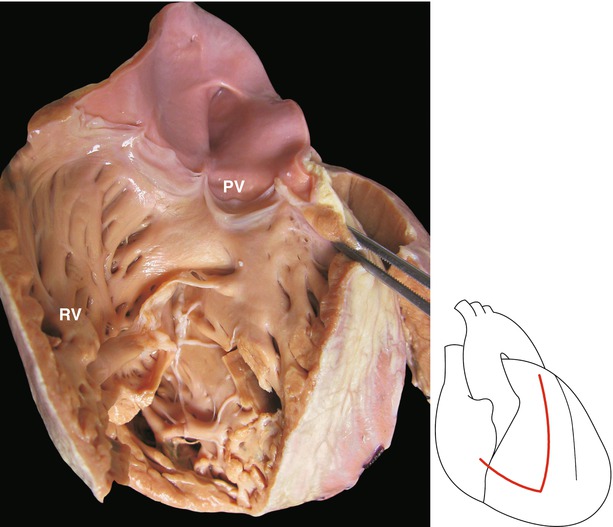
Fig. 2.7
Observation from the anatomical angle. The anterior wall of the RV was incised, and the RVOT was shown. PV pulmonary valve, RV right ventricle
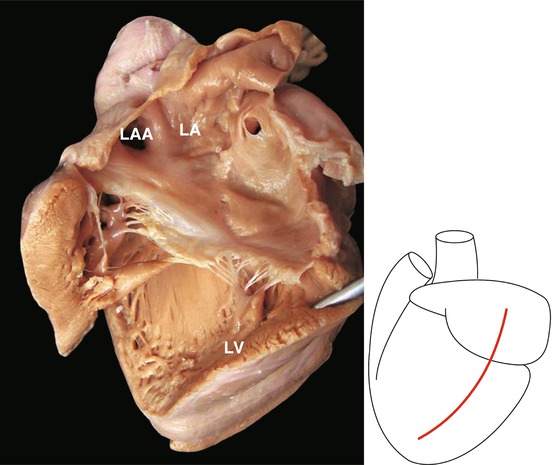
Fig. 2.8
Observation from the left side. The LVOT was shown clearly. LA left atrium, LV left ventricle, LAA left atrium auricle
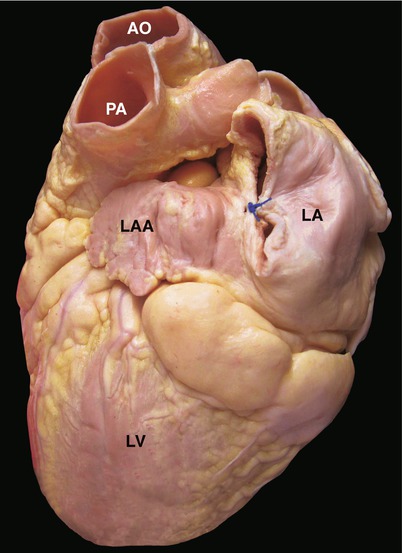
Fig. 2.9
Observation from the left side. AO ascending aorta, LA left atrium, LAA left atrium appendage, LV left ventricle, PA pulmonary artery
Fig. 2.10
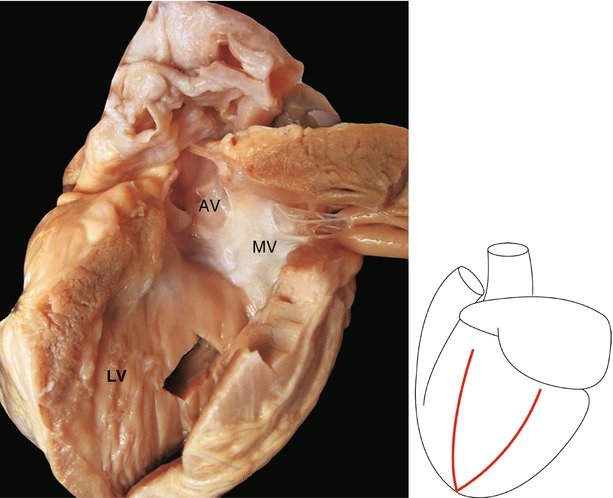
Observation by the left anterior oblique position. The LVOT is exposed, and the MV, AV, and interventricular septum can be seen. AV aortic valve, MV mitral valve, LV left ventricle
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
