(1)
Department of Surgery, Division of Plastic Surgery, University of California, Davis Medical Center, 2221 Stockton Boulevard, Suite 2123, Sacramento, CA 95817, USA
Introduction
Poland’s Syndrome , in the classic sense, is the unilateral absence of the sternocostal head of the pectoralis major muscle, ipsilateral breast hypoplasia, and a concomitant, ipsilateral hand deformity. The syndrome has since evolved to encompass a myriad of anomalies, rarely presenting collectively in the same individual. Consistent in all cases, the congenital absence of the sternocostal head of the pectoralis major muscle is pathognomonic for the disease.
With few exceptions, Poland’s Syndrome represents primarily an aesthetic deformity. Aside from the rare case of cardiopulmonary compromise, surgical intervention is typically delayed until growth is complete. A single-stage approach is preferred, with interdisciplinary collaboration recommended to optimize reconstructive outcomes.
History
In 1841, 19-year-old Alfred Poland provided a detailed account of an unusual anatomic dissection that he performed as a medical student and anatomy apprentice at Guy’s Hospital in London, England. The body was that of 27-year-old convict, George Pelt, who reportedly had difficultly adducting his left arm. Poland’s findings would not only provide an explanation for the condition, but inspire a sketch of the cadaver’s thorax and a preservation of the subject’s hand in the medical museum of Guys Hospital (Fig. 6.1) [1, 2]. Poland’s work was later printed in the Guy’s Hospitals Reports under the title “Deficiency of the pectoral muscles;” [3] and the collection of findings he so astutely described would later serve as the classic description of the syndrome that today bears his name.
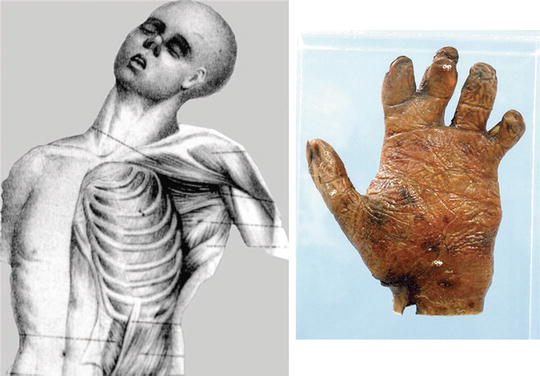
Fig. 6.1
(Left) Illustration made during the 1841 dissection by Alfred Poland and drawn by Poland’s friend, Mr. Tilston. [From Poland, A. Deficiency of the pectoral muscles. GuysHospRep.1841;6:191. Note: Guy’s Hospital Reports went out of print in 1974 [7].] (Right) The left hand of Poland’s 1841 subject as it appears today at the Gordon Museum of Guy’s Hospital, London. The photograph was kindly taken for inclusion [in the article from which this figure was referenced] by William G. J. Edwards, Keeper of the Gordon Museum, Kings College, London, after a recent visit to the museum (and the specimen) by the senior author (A.E.S.) [of the article referenced]. (Used with permission from [2]
It should be noted, however, several reports of similar deformities preceded Poland’s [4–6]. No syndrome or eponym existed at the time; and preceding accounts failed to acknowledge the concomitant hand abnormality. It wasn’t until 1962, over one hundred years later, that Poland’s name was first ascribed to the condition. Patrick Clarkson, a Plastic and Hand Surgeon at Guy’s Hospital, coined the term “Poland’s Syndactyly” to refer to the simultaneous occurrence of breast hypoplasia and syndactyly that he noted in three of his patients [7, 8]. Five years later, Baudinne and colleagues, in their 1967 publication, referred to the complex as “Poland’s Syndrome,” an eponym that continues to this day [9].
Epidemiology
The true incidence of Poland’s Syndrome is difficult to estimate due to the variability with which it presents and the differences that occur in the specific patient cohorts. Most studies indicate an average incidence of 1 in 20,000 to 1 in 30,000 live births, with ranges of 1 in 7000 to 1 in 100,000 reported. It is a condition that lends itself to under-reporting, being a predominantly aesthetic deformity and one that is rather easily concealed. Mammography, providing perhaps a more objective measure, has demonstrated an incidence of 1 in 19,000 [10].
Poland’s Syndrome is most commonly a right-sided, sporadic, congenital deformity. Familial cases have been described, but the incidence of such cases is less than 1 %. Single accounts of bilateral muscle agenesis do exist, and the occasional study demonstrating a left-sided predominance has been reported [11]. Males are affected more frequently than females with a ratio of 2:1 to 3:1. Males show a marked predilection for right-sided involvement; females, in contrast, show much less sidedness. In sporadic cases, the pattern of male and right-sided predominance holds true. In familial cases, however, the incidence in males and females is similar; and the deformity presents equally as common on either side in both genders [10, 11].
Pathogenesis
Although familial cases have been described, Poland’s Syndrome is thought to result from events in utero rather than defined inheritance. Its predominantly unilateral, sporadic occurrence lends support to the idea of an intrauterine insult as the inciting factor. This view is further substantiated by a report of Poland’s Syndrome in only one sibling of a pair of monozygotic twins [10]. The prevailing etiological theory for Poland’s Syndrome favors a vascular origin for the causal intrauterine event.
Bavnick and Weaver suggested the term “subclavian artery supply disruption sequence (SASDS) ” to explain the pathogenesis of a group of syndromes that includes Poland’s Syndrome. They proposed these conditions resulted from an interruption of early embryonic blood supply in the subclavian or vertebral arteries, or their branches, occurring at or around the sixth week of embryologic development. They further hypothesized that occlusion at specific locations within these vessels produced predictable patterns of defects [12].
With respect to Poland’s Syndrome specifically, an early low-flow state to the developing limb bud at the sixth to seventh week of gestation has been suggested with findings of regional vascular hypoplasia corroborating this theory. Decreases in diameter of greater than 50 % and reductions in flow velocity have been demonstrated in the subclavian arteries of patients with Poland’s Syndrome [12–14]. In their case report of an aborted ipsilateral latissimus dorsi flap in a 17-year-old girl with Poland’s Syndrome, Beer et al. present angiographic data demonstrating a hypoplastic, ipsilateral subclavian artery with complete absence of both the ipsilateral thoracoacromial and thoracodorsal branches [15]. Interestingly, the finding of vascular hypoplasia was noted by Alfred Poland, himself. In his initial description, he remarked upon the presence yet diminished size of the thoracic vessels supplying the intercostal spaces [3].
Despite the support for a vascular theory of pathogenesis , skeptics note the sparing of musculoskeletal units on the affected side downstream from the alleged occlusive event as evidence to the contrary of a vascular etiology. An alternative hypothesis is the disruption of the lateral plate mesoderm, from which the pectoralis major muscle develops between 16 and 28 days after fertilization. This disruption has been suggested to account for all defects [10].
The phenotypic mosaicism observed with Poland’s Syndrome has been explained in terms of timing of cell death. A lethal mutation of an upper limb bud cell line has been postulated as the inciting event. Early mutation explains the more severe chest wall and limb defects, whereas, later mutations may produce more localized skin and soft tissue anomalies [11].
Finally, reports of familial cases should not be entirely dismissed. Soltan and Holmes suggested a familial clustering of a common factor (e.g. a vascular abnormality) to describe the occurrence of Poland’s Syndrome in different members of the two sets of siblings who were first cousins [16]. Sujansky et al. proposed a delayed mutation of an autosomal dominant gene to explain the occurrence in two family members related through three unaffected individuals [17]. The delayed mutation theory does appear consistent with these and other reports of familial cases, accurately accounting for both the vertical transmission from parent to child and for cases of affected siblings with unaffected parents.
Clinical Features and Classification
The constellation of clinical features that make up Poland’s Syndrome is quite variable in its presentation. The sine qua non, however, is the congenital absence of the sternocostal head of the pectoralis major muscle . This feature can present alone, or with ipsilateral chest wall and upper extremity deformities. The extent and involvement of each of these components is variable, such that the syndrome is best regarded as a spectrum that varies with the involvement and severity of the constituent anomalies.
A number of classification systems have been described. Seyfer et al. classify the 63 patients in their series as having either “simple” or “complex” Poland’s Syndrome; the “simple” form representing the unilateral absence of the sternocostal head of the pectoralis major muscle, and the “complex” form presenting with the addition of rib and sternal aberrations, muscular displacements, and brachysyndactyly (Figs. 6.2 and 6.3) [2].


Fig. 6.2
Simple form of Poland syndrome. (Left) Illustration of absence of the right sternocostal head of the pectoralis major muscle. (Center) Male patient with right-sided Poland syndrome. (Right) Female patient with left-sided Poland syndrome. Note the asymmetric anterior axillary folds. Both sexes usually express concern about the folds and their chest wall asymmetry. (Used with permission from Seyfer, AE.; Fox, JP.; Hamilton, CG. Poland Syndrome: Evaluation and Treatment of the Chest Wall in 63 Patients. Plast Reconstr Surg. 2010; 126(3):902–911)
Fig. 6.3
Complex form of Poland syndrome in a male patient. (Left) The right hemithorax is smaller and the cartilaginous portions of the upper ribs are absent. With the arms at the side, the axillary fold deficiency is apparent. (Center) The upper extremity components are short and there is a brachysyndactyly (shortened,webbed digits) as described by Poland. (From Seyfer AE, Icochea R, Graeber GM. Poland’s anomaly: Natural history and long-term results of chest wall reconstruction in 33 patients. Ann Surg. 1988;208:776–782. Used with permission). (Right) An axillary web is present, which may represent a forme fruste of the pectoralis major muscle. This webbing, which can also be observed in the simple form, is sometimes contractile. (Used with permission from Seyfer, AE.; Fox, JP.; Hamilton, CG. Poland Syndrome: Evaluation and Treatment of the Chest Wall in 63 Patients. Plast Reconstr Surg. 2010; 126(3):902–911)
Fokin and colleagues divide the syndrome into three groups: “mild (or partial),” “moderate (or classic),” and “severe .” The “mild (or partial)” form is the equivalent of Seyfer’s “simple” designation, representing the sine qua non of the disease. Fokin’s “moderate (or classic)” form and Seyfer’s “complex” form are also similar in that they represent the features originally noted by Poland in his initial report (i.e. pectoralis muscle aplasia, costochondral hypoplasia, and unilateral brachysyndactyly). Fokin adds an additional group of increased severity which he terms the “severe” form; to distinguish those cases that present with the added complexity of lung herniation, latissismus dorsi and deltoid muscle involvement, dextrocardia, ectrodactyly, and/or renal agenesis (Figs. 6.4 and 6.5) [18].
Fig. 6.4
(A–D) Anatomical representation of Poland syndrome. (A) Three-dimensional view. Left-sided rib defect. (B) Cross-sectional view. Rib defect with chest wall depression and shift of the heart to the right. (C) Lateral view. Unilateral chest wall depression. (D) Frontal view. Rib defect and isolated dextrocardia. (Used with permission from Fokin, AA.; Steuerwald, NM.; Ahrens, WA.; Allen, KE. Anatomical, Histologic, and Genetic Characteristics of Congenital Chest Wall Deformities. Semin Thorac Cardiovasc Surg. 2009; 21:44–57)
Fig. 6.5
(A, B) Different degrees of Poland syndrome severity. (A) Partial PS with pectoral muscle deficit only. (B) Full-blown PS with large rib defect, extensive muscle deficit, isolated dextrocardia, and unilateral hand abnormality. (Used with permission from Fokin, AA.; Steuerwald, NM.; Ahrens, WA.; Allen, KE. Anatomical, Histologic, and Genetic Characteristics of Congenital Chest Wall Deformities. Semin Thorac Cardiovasc Surg. 2009; 21:44–57)
Diagnosis
Although the presentation of Poland’s Syndrome is quite variable, the sine qua none for the disease is the congenital absence of the sternocostal head of the pectoralis major muscle. This reflects the simplest and most common form of the syndrome; and is recognized, in either gender, as an absent anterior axillary fold. The female deformity, in its mildest form, manifests with the concomitant finding of breast hypoplasia. The simultaneous occurrence of additional ipsilateral anomalies of the thorax and upper extremity upstage the diagnosis to one of the more severe forms, rounding out the full spectrum of the syndrome.
Prenatal diagnosis is possible by ultrasonic evaluation; but the diagnosis is more commonly made after birth by the constellation of clinical findings [19]. Parents typically notice the severe form of the syndrome early in infancy due to a visibly asymmetric chest wall and brachysyndactyly. The simple form, however, even if known to the patient, may remain hidden from the family until early adolescence when the patient becomes more self-conscious about the asymmetry.
While the majority of patients with Poland’s Syndrome present primarily with an aesthetic concern, in the rare case of cardiopulmonary compromise, severe functional impairment is recognized in infancy and should be addressed with prompt surgical intervention. A thorough assessment of all patients with Poland’s Syndrome is necessary for a complete and accurate diagnosis. Those with the mild form of the syndrome may have measureable differences in the affected hemithorax and upper extremity that may otherwise go unnoticed by visual inspection alone. This also highlights the importance of a thorough examination in individuals presenting with an apparent isolated syndactyly, as up to 10 % of these patients will have Poland’s Syndrome [20].
Physical examination should involve an undraped evaluation of the entire torso and bilateral upper extremities, with inspection, palpation, and measurement of key structural components. This should include measurement of the ribs; as well the distances from sternal notch to acromion, olecranon to ulnar styloid, and lengths of all phalanges; all of which should be compared to measurements on the contralateral, unaffected side. Standard muscle testing is performed, and baseline photographs are taken in the usual fashion [2].
While not a requirement for diagnosis , various imaging modalities may assist with preoperative planning, particularly in cases where autogenous reconstruction is being considered. Computed Topography (CT), Magnetic Resonance Imaging (MRI), and Angiography are the most useful; permitting a more detailed assessment of the skeletal, soft tissue, and vascular anomalies, respectively. Beer et al., in their report of a case of Poland’s Syndrome in a 17-year-old girl, were forced to abort a pedicled latissimus dorsi flap due to severe attenuation of the muscle that was not recognized clinically on preoperative examination. An MRI later confirmed the absence of the latissimus dorsi muscle, with angiography providing the additional findings of subclavian artery hypoplasia and complete absence of its thoracoacromial and thoracodorsal branches. The identification of other coexisting conditions, such as renal agenesis, is another benefit of diagnostic imaging, as this too may affect reconstructive outcomes [15].
Treatment Considerations
The clinical polymorphism Poland’s Syndrome presents with precludes a generalized approach to its surgical management. Rather, an individualized approach is advocated, taking into consideration a number of factors that ultimately influence the therapeutic intervention. The process of arriving at the most appropriate treatment strategy for each patient can be simplified by considering a series of questions provided below:
Does the defect present primarily as a functional or aesthetic concern?
Are there significant psychosocial implications affecting this patient at this time?
Has the patient reached skeletal maturity?
What is the gender of the patient?
What is the severity of the syndrome presentation?
Answers to the first three questions address the issue of timing of intervention, while the latter two provide direction with respect to the particular surgical approach.
Any surgical intervention on the growing child must be viewed as a balance between the benefit of early correction and the risk of future growth impairment. With the deformities in Poland’s Syndrome being predominantly aesthetic in nature, the general consensus is to delay surgical correction until skeletal maturity. Of course, the presence of significant functional deformity trumps the risk of early operative intervention. In Poland’s Syndrome, severe chest wall deformity causing cardiopulmonary compromise, and syndactyly are two such deformities with significant functional implications that warrant early repair. Another exception, one that addresses an aesthetic issue, is the use of tissue expanders in the hypoplastic breast of the skeletally immature patient. By serially expanding the hypoplastic breast to keep pace with the growing contralateral breast, this can minimize asymmetry and the psychosocial implications accompanying this deformity in the adolescent female patient (Fig. 6.6) [21].
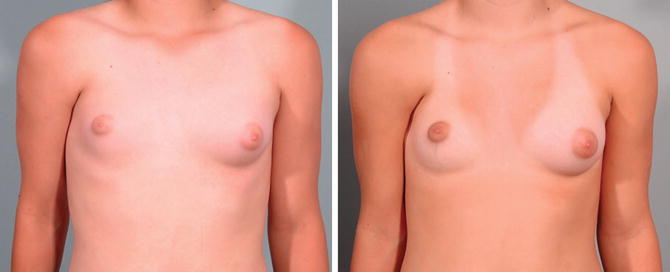
Fig. 6.6
(Left) A 13-year-old girl with mild Poland syndrome. (Right) Result after insertion of tissue expander. The plan is to wait until the patient reaches age 17 years to insert a permanent implant. (Used with permission from Pryor, Landon S.; Lehman Jr., James A., Workmann, Meredith C. Disorders of the Female Breast in the Pediatric Age Group. Plast Reconstr Surg. 2009. 126(1S):50e-60e, 2009)
Aside from the few exceptions provided above, surgical correction of Poland’s Syndrome is delayed until growth is complete. In individuals who have reached skeletal maturity, the particular surgical approach is influenced by patient gender and syndrome severity. The algorithm for both male and female patients is similar, with the obvious distinction that in the female patient the hypoplastic breast is also addressed. Reconstructive needs in the simple and complex forms of the syndrome differ based upon the nature of the musculoskeletal and soft tissue deficiencies present.
The remainder of this chapter will focus on the surgical management of Poland’s Syndrome with a look at the options available for reconstruction of the different forms of the disease. Before we begin, it is worth reviewing the anatomy of the structures typically affected in Poland’s Syndrome, paying particular attention to how the aberrations differ from normal anatomy. An understanding of normal anatomy is paramount if one is to restore normal form in these often-complex defects. Ascribing to fundamental reconstructive principles, we shall take an inside-out approach, beginning with a look at thoracic skeleton.
Anatomy
Thoracic Skeleton
The normal thoracic skeleton is an osseous cage comprising the sternum, the thoracic vertebrae, 12 pairs of ribs and the clavicles. It houses and protects the heart, lungs, and great vessels of the thorax; serves as a major structural support for the body and upper extremities; and contributes to respiratory function. In the simple (partial or mild) form of Poland’s Syndrome, the osseous thorax is entirely normal; the more advanced forms present with rib and sternal aberrations. If these aberrations are severe enough to compromise pulmonary function or protection of the heart, surgical intervention is undertaken early irrespective of skeletal maturity.
Patients with rib and sternal involvement characteristically present with a sunken chest on the affected side (Fig. 6.7). This is caused by hypoplasia of the ribs and cartilages in the moderate form (Fig. 6.8), and aplasia of the anterior portion of the ribs and cartilages in the severe (complete) form of the disease (Fig. 6.9). One to three ribs are typically affected. Ribs 1–3 and ribs 2–4 are the most commonly affected groups, the latter occurring more frequently than the former. In the case of rib aplasia, the sternal ends of the aplastic ribs may be entirely separate or fused together [10].
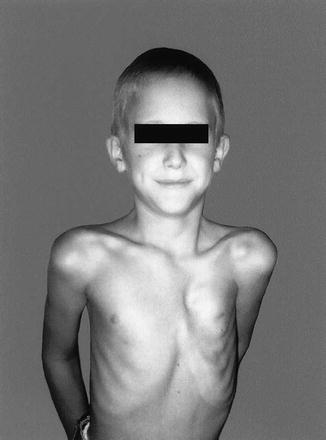
Fig. 6.7
Photograph of a patient with Poland’s syndrome. (Used with permission from Fokin, AA.; Robicsek, F. Poland’s Syndrome Revisited. Ann Thorac Surg. 2002; 74:2218–2225)
Fig. 6.8




Chest involvement in moderate form of Poland’s syndrome. (A) Three-dimensional, oblique view showing chest wall depression with hypoplasia of ribs III to V. Mild rotation of the sternum. (B) Cross-sectional view showing normal position of the heart between the sternum and vertebral column. (C) Lateral view showing unilateral depression of the ribs. (D) Frontal view showing hypoplasia of the involved ribs. Normal position of the heart. (Used with permission from Fokin, AA.; Robicsek, F. Poland’s Syndrome Revisited. Ann Thorac Surg. 2002; 74:2218–2225)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
