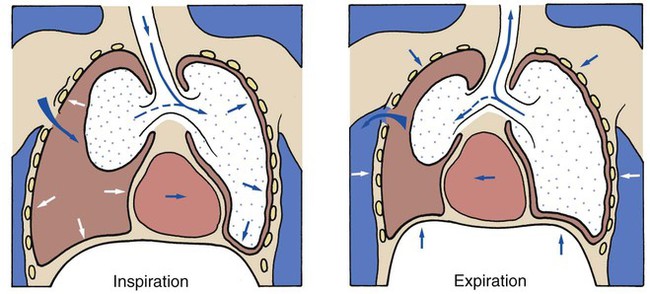
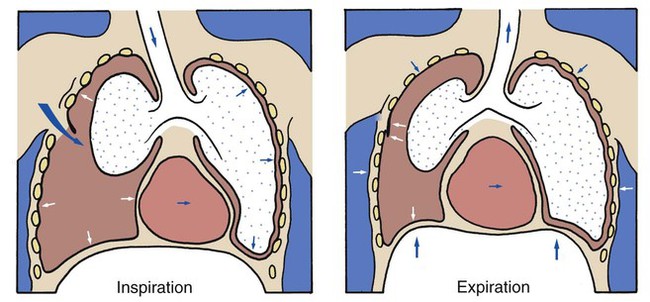
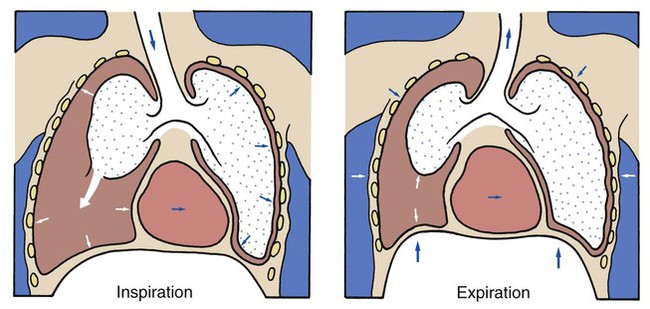
After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with a pneumothorax. • Describe the causes of a pneumothorax. • List the cardiopulmonary clinical manifestations associated with a pneumothorax. • Describe the general management of a pneumothorax. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. A pneumothorax exists when gas (sometimes called free air) accumulates in the pleural space (see Figure 22-1). When gas enters the pleural space, the visceral and parietal pleura separate. This enhances the natural tendency of the lungs to recoil, or collapse, and the natural tendency of the chest wall to move outward, or expand. As the lung collapses, the alveoli are compressed and atelectasis ensues. In severe cases, the great veins may be compressed and cause the venous return to the heart to diminish. Gas can gain entrance to the pleural space in the following three ways: 1. From the lungs through a perforation of the visceral pleura 2. From the surrounding atmosphere through a perforation of the chest wall and parietal pleura or, rarely, through an esophageal fistula or a perforated abdominal viscus 3. From gas-forming microorganisms in an empyema in the pleural space (rare) Penetrating wounds to the chest wall from a knife, a bullet, or an impaling object in an automobile or industrial accident are common causes of traumatic pneumothorax. When this type of trauma occurs, the pleural space is in direct contact with the atmosphere, and gas can move into and out of the pleural cavity. This condition is known as a sucking chest wound and is classified as an open pneumothorax (Figure 22-2). A piercing chest wound also may result in a closed (valvular) or tension pneumothorax through a one-way valvelike action of the ruptured parietal pleura. In this form of pneumothorax, gas enters the pleural space during inspiration but cannot leave during expiration because the parietal pleura (or, more infrequently, the chest wall itself) acts as a check valve. This condition may cause the intrapleural pressure to exceed the atmospheric pressure in the affected area. Technically this form of pneumothorax is classified as a tension pneumothorax (Figure 22-3). This form of pneumothorax is the most serious of all. When a pneumothorax occurs suddenly and without any obvious underlying cause, it is referred to as a spontaneous pneumothorax. A spontaneous pneumothorax is secondary to certain underlying pathologic processes such as pneumonia, tuberculosis, and chronic obstructive pulmonary disease (COPD). A spontaneous pneumothorax is sometimes caused by the rupture of a small bleb or bulla on the surface of the lung. This type of pneumothorax often occurs in tall, thin persons aged 15 to 35 years. It may result from the high negative intrathoracic pressure and mechanical stresses that take place in the upper zone of the upright lung (Figure 22-4). A spontaneous pneumothorax also may behave as a tension pneumothorax. Air from the lung parenchyma may enter the pleural space via a tear in the visceral pleura during inspiration but is unable to leave during expiration because the visceral tear functions as a check valve (see Figure 22-4). This condition may cause the intrapleural pressure to exceed the intraalveolar pressure. This form of pneumothorax is classified as both a closed pneumothorax and a tension pneumothorax. The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8)—the major anatomic alteration of the lungs associated with pneumothorax (see Figure 22-1). CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE Increased Respiratory Rate (Tachypnea) Stimulation of Peripheral Chemoreceptors (Hypoxemia) If the patient has a pneumothorax as a result of a sucking chest wound, an additional mechanism also may promote hypoventilation. In other words, when a patient with this type of pneumothorax inhales, the intrapleural pressure on the unaffected side decreases. As a result the mediastinum often moves to the unaffected side, where the pressure is lower, and compresses the normal lung. The intrapleural pressure on the affected side also may decrease, and some air may enter through the chest wound and further shift the mediastinum toward the normal lung. During expiration the intrapleural pressure on the affected side rises above atmospheric pressure, and gas escapes from the pleural space through the chest wound. As gas leaves the pleural space, the mediastinum moves back toward the affected side. Because of this back-and-forth movement of the mediastinum, some gas from the normal lung may enter the collapsed lung during expiration and cause it to expand slightly. During inspiration, however, some of this “rebreathed dead space gas” may move back into the normal lung. This paradoxic movement of gas within the lungs is known as pendelluft. As a result of the pendelluft, the patient hypoventilates (see Figure 22-2). As a result of the reduced alveolar ventilation, the patient’s
Pneumothorax
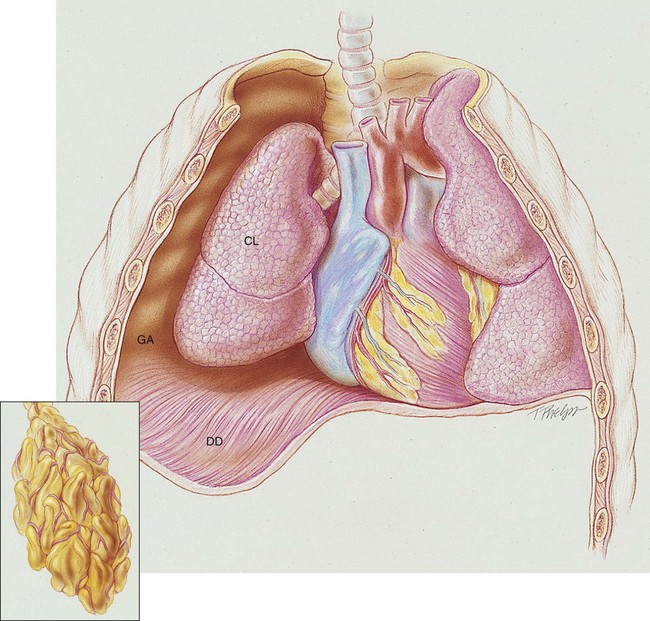
Anatomic Alterations of the Lungs
Etiology and Epidemiology
Traumatic Pneumothorax
Spontaneous Pneumothorax
Iatrogenic Pneumothorax
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pneumothorax
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pneumothorax
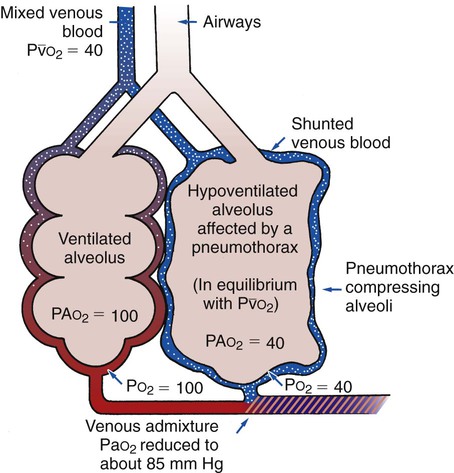
 ratio decreases. This leads to intrapulmonary shunting and venous admixture (Figure 22-5). Because of the venous admixture, the Pao2 and Cao2 decrease. As this condition intensifies, the patient’s arterial oxygen level may decline to a point low enough to stimulate the peripheral chemoreceptors. Stimulation of the peripheral chemoreceptors in turn initiates an increased ventilatory rate.
ratio decreases. This leads to intrapulmonary shunting and venous admixture (Figure 22-5). Because of the venous admixture, the Pao2 and Cao2 decrease. As this condition intensifies, the patient’s arterial oxygen level may decline to a point low enough to stimulate the peripheral chemoreceptors. Stimulation of the peripheral chemoreceptors in turn initiates an increased ventilatory rate.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree