Pneumomediastinum
Jonathan H. Chung, MD
DIFFERENTIAL DIAGNOSIS
Common
True Pneumomediastinum
Alveolar Rupture
Tracheobronchial Injury
Esophageal Injury
Iatrogenic Injury
Extension from Neck or Abdomen
Mediastinitis (Rare)
Medial Pneumothorax (Mimic)
Mach Band (Mimic)
Less Common
Pneumopericardium
Skin Fold (Mimic)
Paratracheal Air Cyst (Mimic)
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
CT generally diagnostic in differentiating pneumomediastinum from its mimics
Helpful Clues for Common Diagnoses
True Pneumomediastinum
Alveolar rupture due to asthma, coughing, Valsalva maneuver, volutrauma, alveolar lung disease, or interstitial lung disease
Iatrogenic injury due to chest tube placement or tracheostomy
Ectopic gas in mediastinum; often clinically evident
Lucency along heart border that often extends into neck; lucent regions around mediastinal structures
Continuous diaphragm sign: Gas outlines inferior aspect of heart (also in pneumopericardium)
Medial Pneumothorax (Mimic)
Pneumothorax in other portions of pleural space
If not loculated, will rapidly shift with change in position
Mach Band (Mimic)
Lacks distinct pleural line of pneumomediastinum
Artifact no longer apparent when excluding dense heart from field of vision
Helpful Clues for Less Common Diagnoses
Pneumopericardium
Does not extend above level of hila; continuous diaphragm sign
Rapidly shifts with change in position
Skin Fold (Mimic)
Lacks distinct pleural line of pneumomediastinum; may see indistinct black line (gas in skin fold)
Often nonanatomic orientation; disappears on repeat studies
Paratracheal Air Cyst (Mimic)
Small gas-filled foci at thoracic inlet along right posterolateral aspect of trachea
Connection to trachea rarely seen
Image Gallery
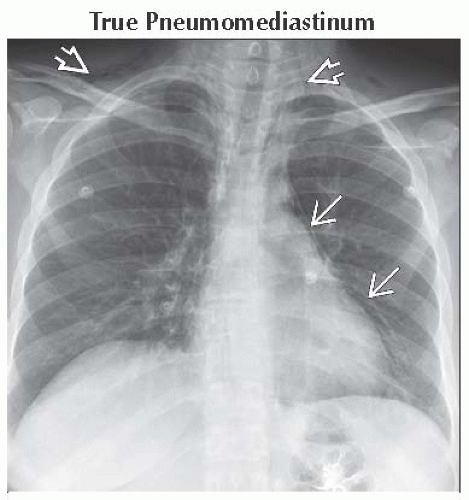 Frontal radiograph shows lucent regions along the left aspect of the mediastinum
 extending into the neck and shoulders extending into the neck and shoulders  , highly suggestive of pneumomediastinum. , highly suggestive of pneumomediastinum.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|