Fig. 10.1
Measuring the pressure correcting the deformity by the help of “compression test device”
Orthosis Treatment
If the pressure test results are less than 10 kg, the patients may benefit from (compressive) orthotic bracing which generally lasts 6 months. The patients have to wear custom-made orthotic brace all the day through (Fig. 10.2). Orthosis is suggested for children older than 5 years old due to the problem of coherence. If the deformity persists more than 6 months, orthosis therapy may prolong for 9–12 months.

Fig. 10.2
Custom-made orthotic brace
Preoperative Evaluation and Preparation
Postero-anterior and lateral chest radiograms and photos of the patient in six different angles of the thoracic cavity are taken. Routine laboratory analysis, ECG and pulmonary function tests are performed. We do not routinely perform echocardiography and thoracic computed tomography unless complicated anomalies are suspected.
The bar used for MIRPC operation is metalic composition of nickel and steel (Fig. 10.3). If the patient is allergenic for metals, it is not appropriate to use this bar. In these kind of cases, we prefer inserting titanium bars instead of standard ones. Detailed patient history and allergy skin test is useful for identifying the metal allergy. We order special titanium bars for the allergenic patients [13–16].
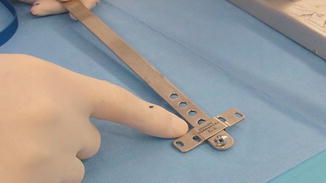
Fig. 10.3
Bar and stabilizer of pectus carinatum
Surgical Technique
Patients are positioned in supine position with both arms abducted and then are entubated by single lumen tracheal tube. Maximal protrusion area is the path of the bar. Mid-axillary lines, where edges of the bar will be placed bilaterally, is identified with marker pen. Mid-axillary lines will also be marked for the right place of the stabilizers. The length of the bar is designated according to this path. Templates (aluminium models) are used for designating the proper bar size. We compress the chest wall until the desired appearance is obtained. The carinatum bar, which is in same size with the model, is formed according to template. After bending the carinatum bar, the surgeon starts with 3 cm long incisions on mid-axillary lines bilaterally and prepares space for stabilizers under serratus anterior muscle. After dissection of the muscles, two parallel ribs are chosen where stabilizers will be fixed by the help of the hook. One centimeter incision is made on the periosteum of the chosen ribs and the periosteum is dissected. A hook is placed around the rib subperiostally and a suction catheter is attached to the tip of the hook and the hook is pulled back with the catheter (Fig. 10.4). A sternal cable (Pioneer Sternal Cable System, Marquette, MI) (if unavailable, two to three times folded no: 5 steel wire) is passed through the suction catheter which is around the rib using it as a guide for fixing the stabilizer. This procedure is repeated on both sides on each ribs. When wrapping up with the wires are completed, stabilizers are fixed to ribs. Long aortic clamps are used to make tunnel under the muscles for the insertion of the bar. Then introducer is inserted through tunnel. By the help of the introducer, a 28 Fr thorax drain is passed through the tunnel as a guide. The bar is attached to the drain and both are pulled back from the tunnel. The bar is placed into the tunnel over the sternum and the edges are slipped into the stabilizer. Bar is fixed to the stabilizer in proper position by the help of clips (Fig. 10.5). 2/0 vicryl sutures are used to cover the muscle fibers over the stabilizers and edges of the bar. Subcutaneus tissue is closed continuously by 2/0 vicryl and cutaneous tissue by 5/0 monocryl sutures.
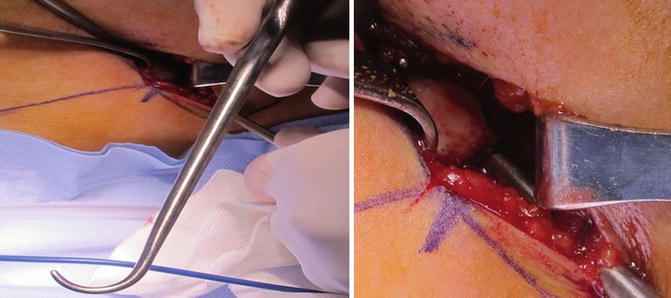
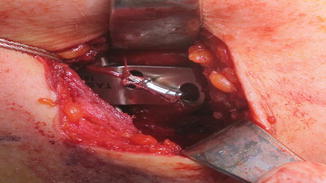
Fig. 10.4
Hook used to turn around (girdle) the rib
Fig. 10.5
Fixing the stabilizer to the ribs by wires
Postoperative Period
Pain is the most serious problem just after the operation. Pain is due to stabilizers, which are placed subperiostally with wires, can be relieved with intravenous (iv) analgesics. IV “Patient Controlled Analgesia (PCA)” is the preferred method for these patients.
Patients are mobilized 6 h after the operation. Analgesics are terminated on 3rd or 4th postoperative day and discharged with oral analgesics on 5th day. Patients can go back to school or work after 2–3 weeks rest at home. It is advised to lie back for the first month and participate in active sports for 3 months.
Early and Late Complications
Pneumothorax and wound infection are the most frequent complications in early postoperative period. Physicians operating MIRPC always have to keep in mind that surgery is based on implanting foreign body into the patient. Antibiotherapy for prophylaxis and postoperative period with close care reduces infection rates less than %1 [17].
If secondary infection occurs, it can be treated by drainage, proper antibiotherapy and even in some serious cases removal of the bar may be necessary.
Late complications are basically breakage of wires that are holding the stabilizers, infection, erosion of the skin, hyperpigmentation, late allergic reactions, cutaneous adhesion and insufficient correction.
Wire breakage is an important late complication as well. We can make two or three fold spiral wires to prevent this complication. In our series we used sternal cable (Pioneer Sternal Cable System, Marquette, MI) and avoided the risk afterwards.
Proper patient selection, respiratory physiotherapy, prophylactic antibiotherapy and most importantly progress with experience in the operation have great benefit on decreasing complications.
Results
Results for MIRPC in long lasting period is almost satisfactory on different series [18]. In our series of 140 cases, questionnarie of patient satisfaction was perfect except three patients.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


